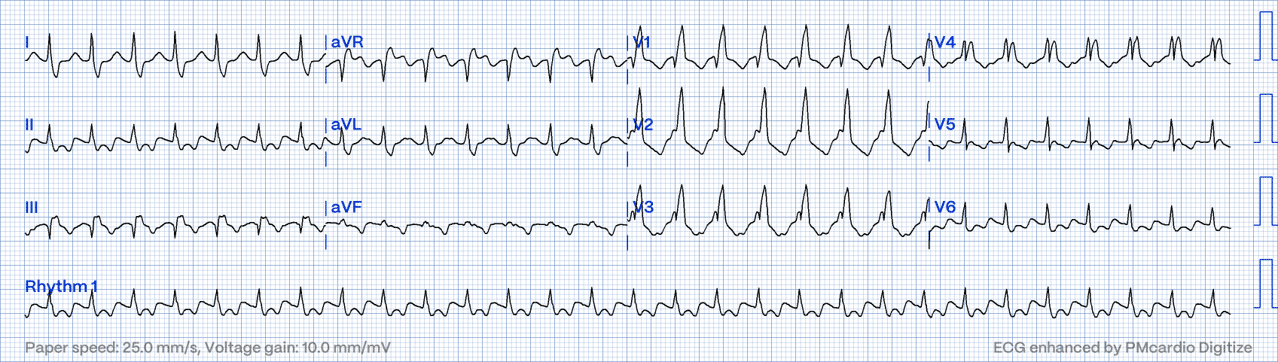
This ECG was AVJRT with RBBB aberrancy.
Aberrancy is the phenomenon where SVT overwhelms the His-Purkinjie system, resulting in rate related bundle branch block (the heart rate is too fast for the bundle branch to recover). Most commonly, Aberrancy results in RBBB, since the Right Bundle Branch generally has a longer recovery time than the left bundle branch.
Although there are various algorithms for differentiating VT vs SVT with aberrancy, I find a simpler approach is a good starting point. Put simply, SVT with aberrancy can be suspected when the ECG looks identical to a bundle branch block. This requires a strong knoweldge of bundle branch block ECG features.
Lets take a look at some of the features of this ECG that points towards aberrancy rather than VT.
1. Exact RBBB features: V1-V3 are dominantly positive with observable rSR complexes (with left r smaller than right R) in typical fashion of Right bundle branch block (RBBB).
2. VT features are absent. Examples of features that are NOT present:
3. Potential P wave activity: The mid RP notches in V4, and the terminal r’ wave of the V5 QRS are suspicious of P wave activity (blue arrows). However, their respective timing relative to the QRS, are inconsistent to one another. Without more information, it is difficult to be sure which one of these (if either of them) are the true P waves.
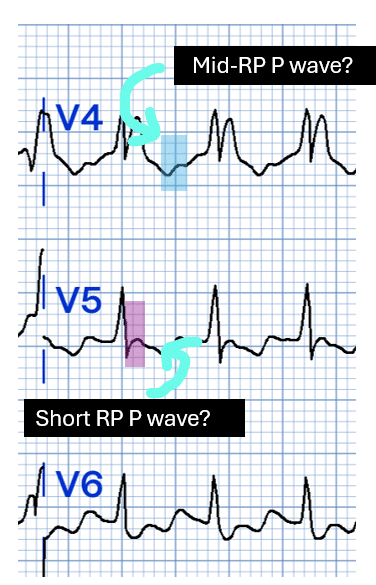
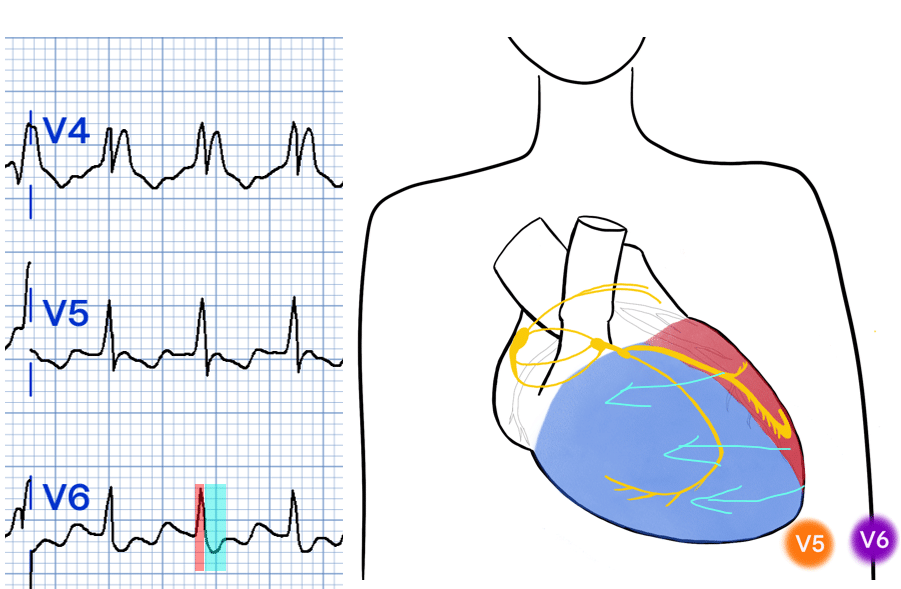
This ECG was AVJRT with RBBB aberrancy, and so it is likely that the terminal r’ wave in V5 represented a retrograde P wave as typical AVJRT is a short RP tachycardia.
My Two Cents:
I have a fairly simple perspective on differentiating VT vs Aberrancy. Firstly, I have become very familiar with the ECG features of RBBB, LBBB and fascicular blocks.
Secondly, if the ECG perfectly looks like a bundle branch block, it probably IS a bundle branch block and therefore aberrancy (unless there is reason to suspect bundle branch reentry VT or fascicular VT which can perfectly mimick bundle branch/fascicular aberrancy).
If the ECG doesn’t look like a perfect bundle branch block, then VT is most likely, remembering that 80% of undifferentiated wide complex tachycardias are VT, especially in the context of known cardiac disease which can act as substrate for VT.
Simply put, if it looks like a perfect bundle branch block, then it probably is (aberrant). If it does not look like a perfect bundle branch block, then it probably isn’t and therefore VT.
This post will be the first of many on this subject. It’s a good starting point, & is a philosophy that has served me well, but there’s still much more to discuss in the future.
Thanks for tuning in :)
Cheers
Mitch & CPP Team
Greater detail on SVT with Aberrancy Vs VT can be found in our ECG course