Answer:
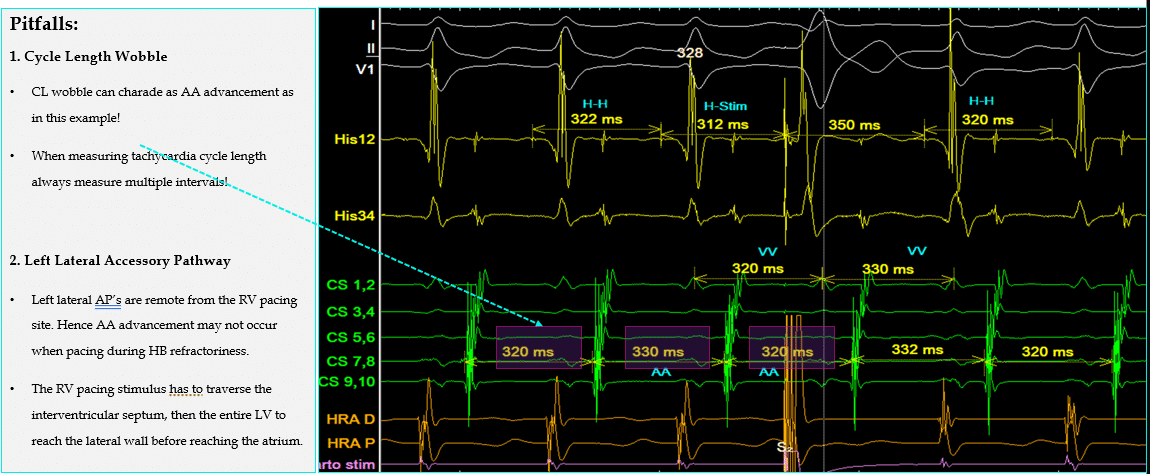
Positive Zipes/His-Synchronous RV Pacing with AA advancement & subsequent VV perturbation indicating Accessory pathway mediated tachycardia (AVRT).
His-Synchronous RV Pacing/Zipes
Also known as “Zipes,” is a valuable maneuver for confirming the presence of accessory pathway-mediated tachycardia (AVRT). This technique is particularly useful when an accessory pathway is suspected and needs confirmation.
Ensuring His-Synchronicity:
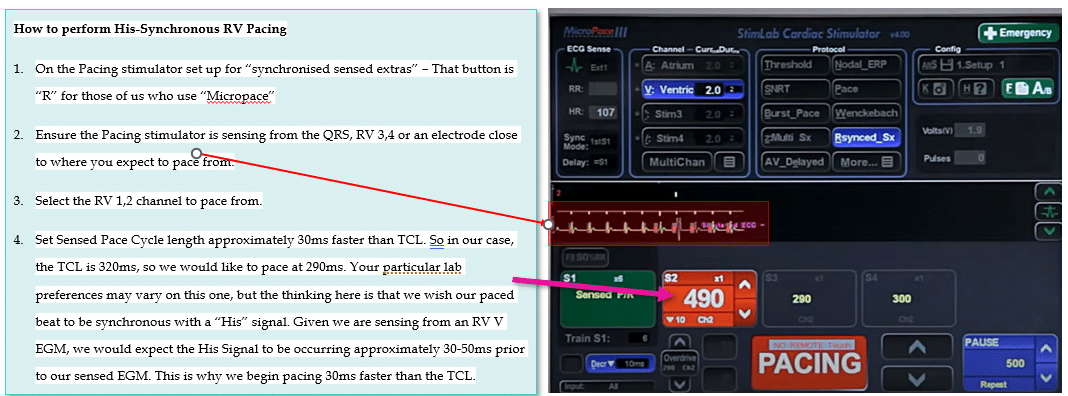
Crucially, we must ensure the RV paced stimulus is “His-Synchronous,” as the maneuver is invalid otherwise.
To ensure the RV paced stimulus is “His-Synchronous” (crucial for a valid maneuver), follow these steps:
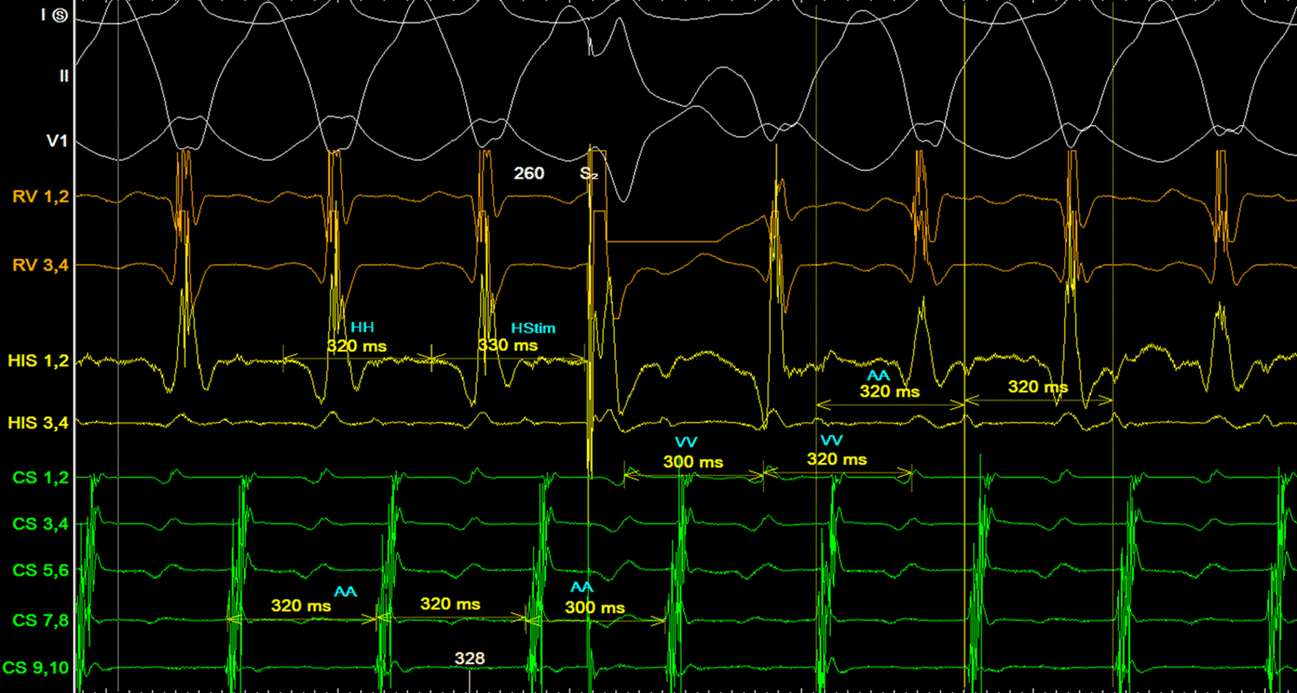
In the example below, H-Stim – HH interval = +10ms, so we can be fairly certain that our RV paced beat is TRULY “His Synchronous”.
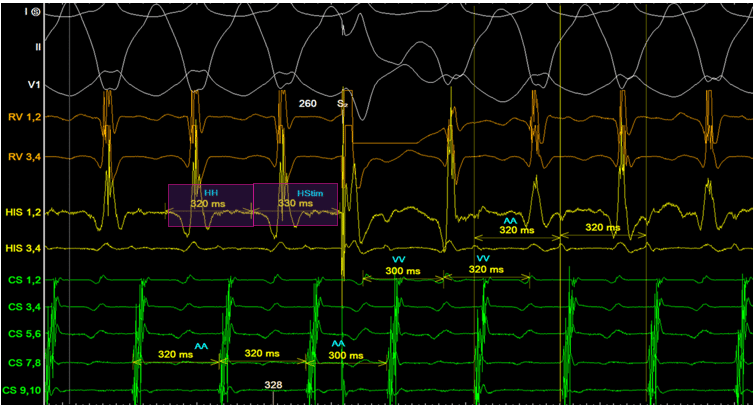
Side note: I admit that our “His” signal in this example is pretty dodgy. That is no criticism of the operator; it happens to the best of them. Ideally, you have a clearer His signal than this. You’re going to have to trust me that HH measurement is really measuring a sneaky His signal.
What to measure?
We are interested in measuring just x2 things:
There are x3 possible outcomes & conclusions – many forget to differentiate the 2nd & 3rd result
1. No perturbation of either immediate AA interval or subsequent VV interval.
Conclusion: No evidence of Accessory pathway. NOTE: The absence of evidence is NOT evidence of absence.
2. Perturbation of immediate AA interval >10ms (advancement or delay), with no change in subsequent VV interval.
Conclusion: Indicates an accessory pathway, but not its participation in tachycardia. This could suggest a bystander pathway.
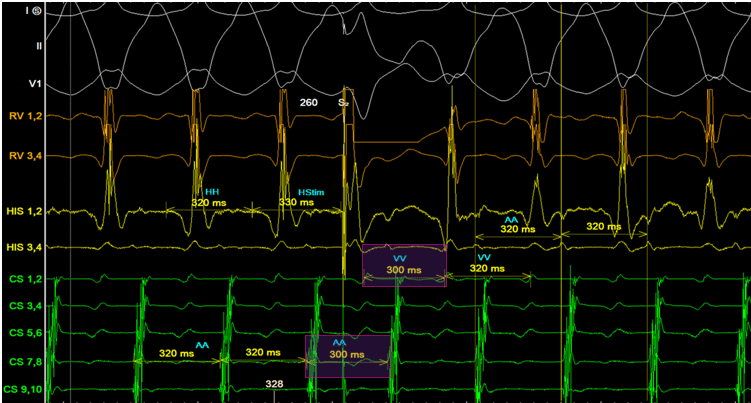
3. Perturbation of both immediate AA & subsequent VV interval by >10ms.
Conclusion: This confirms both the presence AND participation of the accessory pathway in tachycardia. Diagnostic of AVRT.
In the example above, we observe a 20ms AA Advancement, confirming the presence of an accessory pathway. Furthermore, the subsequent VV interval advances by 20ms, indicating participation in SVT.
My Two Cents:
Due to the possibility of a “null” result, for SVT’s which appear more like AVJRT or Focal AT, RV overdrive pacing (entrainment) is probably more useful as it consistently provides useful data, irrespective of the result, so long as entrainment has been achieved.
Thanks for tuning in
Cheers
Mitch & CPP Team
Some extra pitfalls mentioned below :)
We have more detailed explanations on SVT differentiation manoeuvres in our EP in Practice Program 2: SVT in EP.