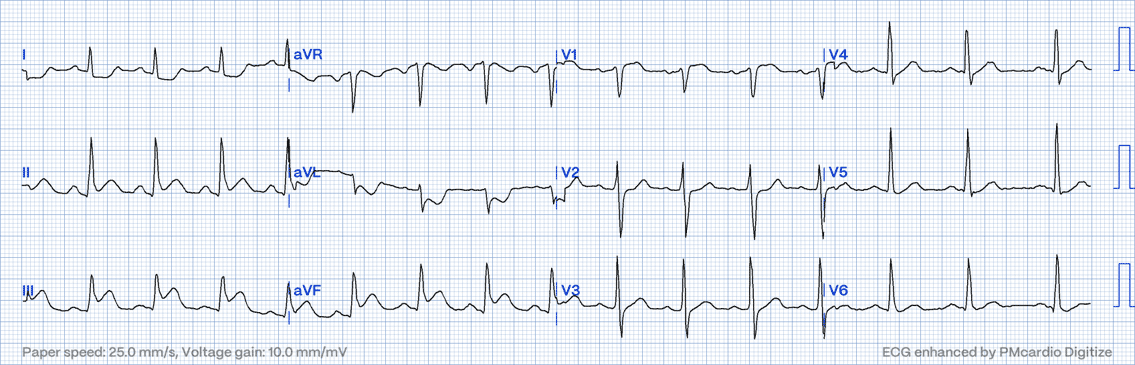
Sinus rhythm with inferior MI & likely RV involvement. This patient had an occluded proximal RCA which was treated with emergency PCI.
Detection & explanation
ST elevation in leads II, III, aVF & V1, with high lateral depression (I & aVL)
The Right Ventricle is supplied by the RV marginal branch which branches off the mid RCA in most cases. This means that proximal or mid-RCA occlusions can also result in RV infarction & occur in approximately one-third of patients who have an inferior MI (of the LV).
Pathophysiology of RV infarction:
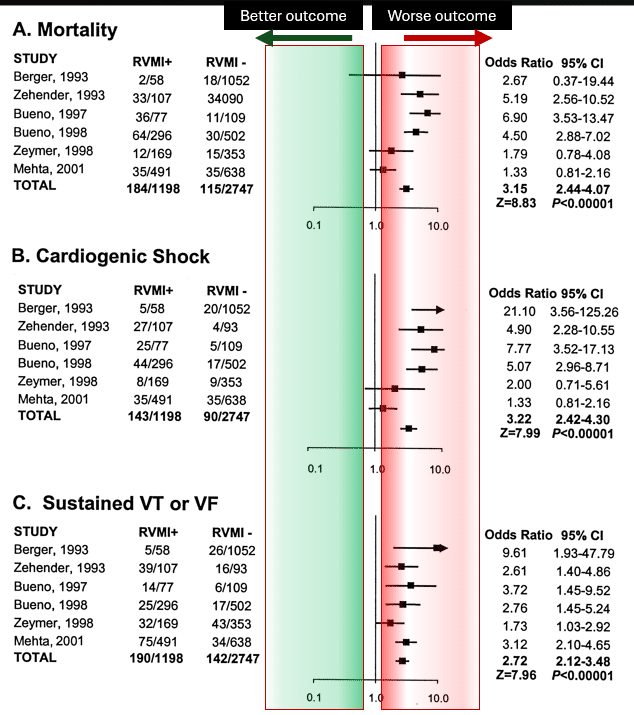
Prognosis of inferior MI with RV involvement vs no RV involvement
My two cents:
Inferior MI with concurrent RV infarction is a serious diagnosis with an almost 3-fold increase in mortality & is associated with a large territory of injury. The physiology of RV MI, predisposes to haemodynamic collapse & resulting brady & tachyarrhythmias. Concurrent RV infarction can most often be suspected when inferior ST elevation occurs concurrently with V1 elevation & high lateral depression, with lead III ST elevation > lead II.
Thanks for tuning in :)
Cheers
Mitch & CPP Team
More on inferior LV & RV MI can be found in ECG in Practice Program 1
https://cardiacphysinpractice.com/ecg-in-practice/