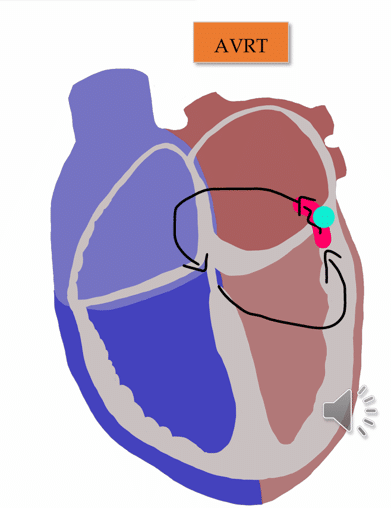
Answer: Orthodromic AVRT.
Differentiating the mechanism of SVT has implications for medical therapy, & ablation strategy.
A regular narrow complex tachycardia in a young patient is most likely AVJRT, AVRT, or Focal AT, listed from most to least likely. Both AVRT and AVJRT are common across genders and age groups, but AVRT is more prevalent in young males in their teenage years, while AVJRT is more frequent in females aged 20-40 years.
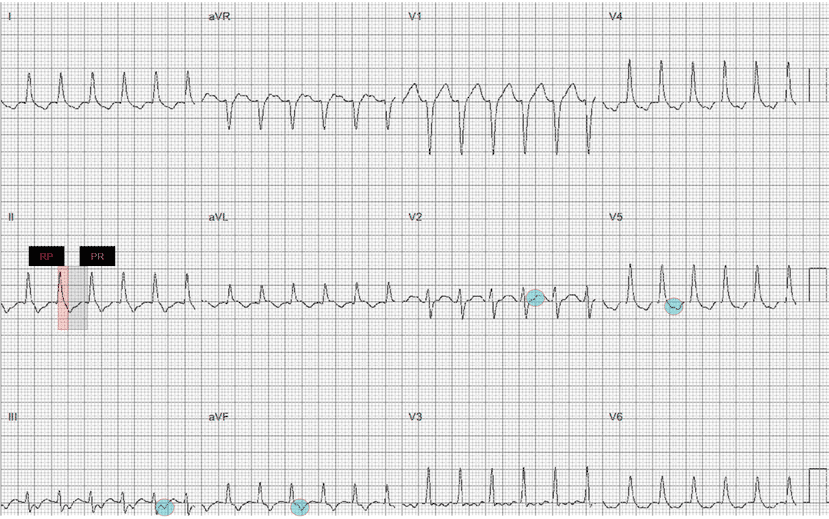
To diagnose the specific SVT, we need to identify P waves and determine if it is a short or long RP tachycardia.
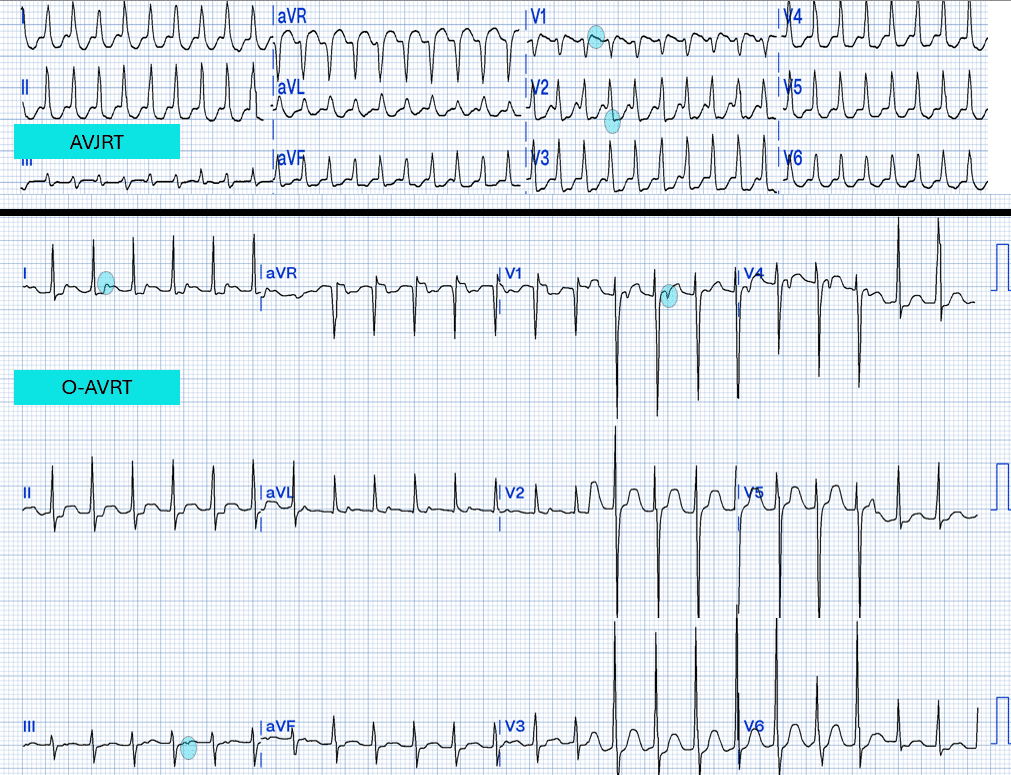
Now that we have established it is a short RP SVT, we need to differentiate between AVJRT and AVRT.
My two cents:
In combination with knowledge on demographic & symptom profile, establishing the RP interval can help predict the mechanism of SVT & arrive at a specualtive diagnosis.
In this case, a young male presenting with a short RP interval, where the RP interval is within the ST segment rather than the QRS complex. The demographic & location of the P wave is most indicative of orthodromic AVRT as the diagnosis.
An even shorter RP would suggests AVJRT, whereas a long RP would suggest Focal AT unless there were other factors which suggested re-entry as the mechansim such as the mode of SVT initiation (a subject for a later Beat Box tune!).
Thanks for tuning in :)
Cheers
Mitch & CPP Team
For more information, check out either our ECG course here, or our intro to EP here,or SVT in EP here.