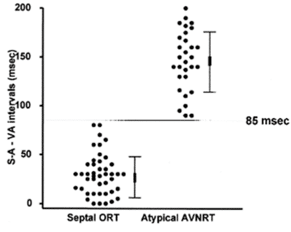
VAVA response excludes Focal AT, indicating likely AVJRT(AVNRT) or AVRT. In the absence/addition to a measured Post Pacing Interval (PPI –TCL), the SA – VA measurement can be used where the Stim-HRA time during RV apex pacing is compared to the VA time during tachycardia to differentiate between AVJRT & AVRT.
How do we use SA – VA measurements?
In this example, the SA – VA = 150ms, lending evidence to AVJRT rather than AVRT.
How does the SA – VA manoeuvre work?
This is because RV pacing VA conduction involves “sequential” conduction through the distal His-Purkinje system, up the RV septum & through the AV node. On the other hand, during AVJRT, VA conduction is simply via the AV node and does not involve the RV septum & the distal His Purkinjie system (The VA time is a pseudo-interval in AVJRT). Hence, during AVJRT, VA conduction is significantly shorter when compared to pacing from the RV apex.
When does SA-VA let you down?
My Two Cents:
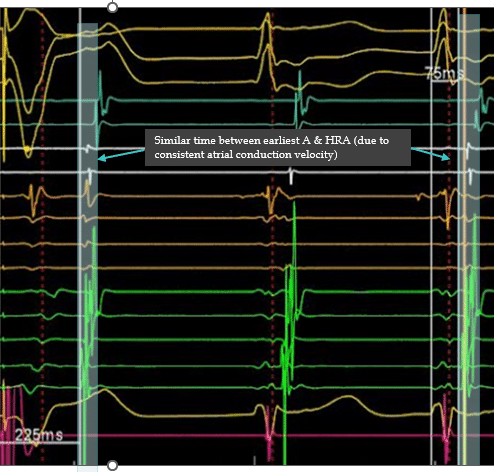
SA – VA is a staple manourve in the EP lab. It is also low hanging fruit, because it can be performed without sustained tachycardia & in the absence of successful entrainment. Perhaps a controversial opinion, but unless patients are exhibiting marked variability in intra-atrial conduction velocity, I honestly think using a consistent Atrial EGM is a reasonable substitute for using a HRA EGM if needed. For these reasons, it is an incredibly versatile measurement and there are few reasons not to routinely consider it when differentiating SVT.
Thanks for tuning in :)
Cheers
Mitch & CPP Team
Further explanation, details & examples can be found in:
EP in Practice – Program 2
Michaud G, Tada H, Chough S, et al. Differentiation of atypical atrioventricular node re-entrant tachycardia from orthodromic reciprocating tachycardia using a septal accessory pathway by the response to ventricular pacing. J Am Coll Cardiol. 2001 Oct, 38 (4) 1163–1167.