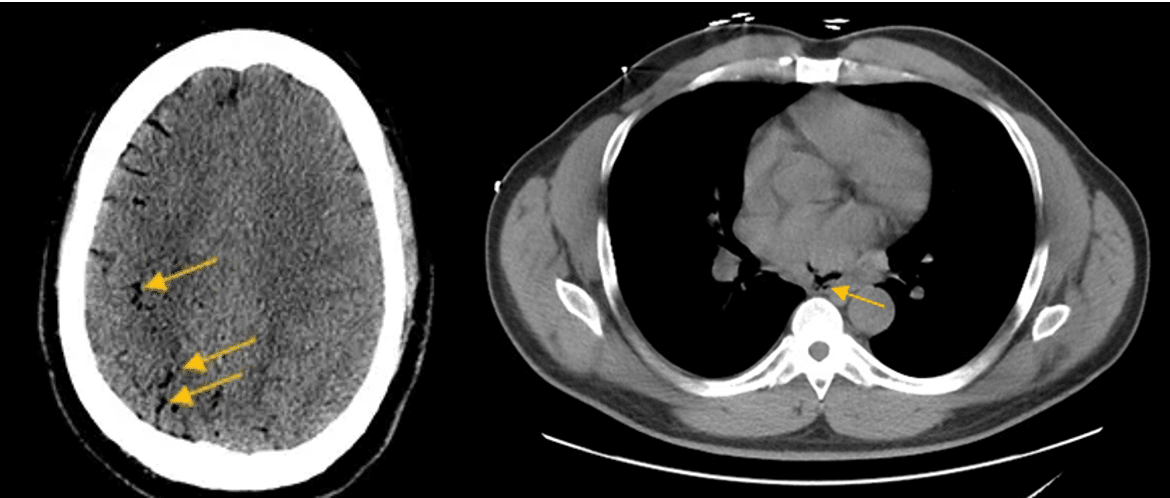
A 61-year-old male presents to ED with fever & neurological symptoms suggestive of stroke. History of hypertension, previous PCI for stable angina 7 months ago and previous AF ablation 3 weeks ago. CT scans of his brain & chest demonstrate some unusual findings below. What is a possible cause of his symptoms?
(Click to zoom on image)
Answer:
Click to Show Answer
Answer: Atrio-oesophageal fistula resulting in stroke & fever. Pockets of air can be visualised in the brain & left atrium, contributing to neurological deficits. Fever caused by oesophageal foreign material entering heart & systemic circulation.
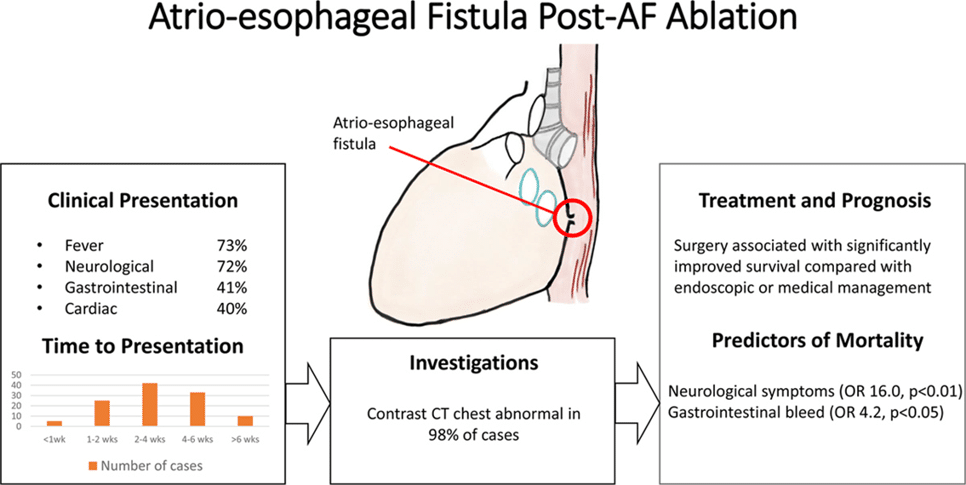
Fever and neurological symptoms are the most common presentation as a result of air emboli entering the brain & foreign material entering the heart/systemic circulation. Vomiting of blood (“hematemesis”) is also a common presentation.
Prevalence
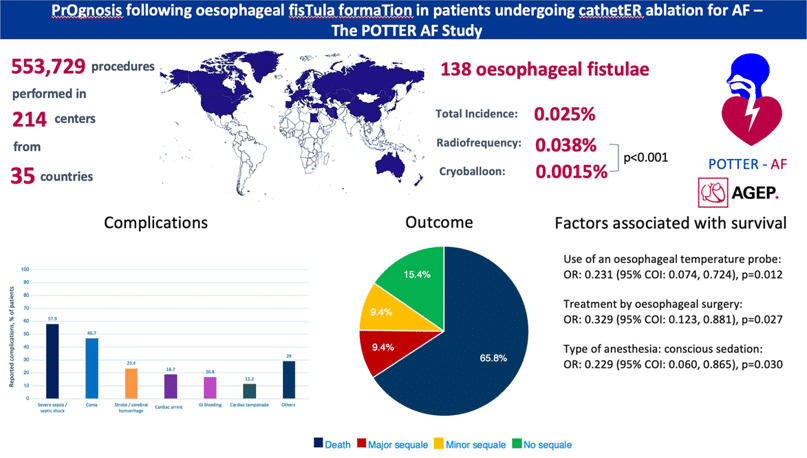
Overall, this complication is rare, occurring in <1 in 4000 procedures (RF & Cryo) worldwide with the POTTER-AF study reporting a mortality of 90% without surgical intervention, & 60% with surgical intervention.
Mechanism of OesophagealInjury
The exact mechanism of oesophageal injury & fistula formation may be through one of or a combination of the following mechanisms:
Direct thermal injury to the oesophageal mucosa resulting in wall thinning, necrosis & eventual perforation.
Thermal injury to arterial supply of oesophagus, resulting in progressive oesophageal ischemic injury, subsequent wall thinning & eventual perforation.
Injury to nervous & vagal supply to oesophagus, pyloric sphincter & gastric antrum may result in oesophageal & gastric dysmotility & pyloric sphincter dysfunction. This can result in oesophageal reflux, contribute to oesophagitis & may eventually contribute to perforation risk in subsequent weeks after ablation procedure.
PFA is “safe”??
Conceptually, PFA should cause less thermal insult to the oesophagus than RF or Cryo although it is difficult to quantify by how much because it is such a rare complication.
Smooth muscle such as oesophageal muscle has a higher electroporation threshold for ablation/injury compared to myocytes. This makes it conceptually possible to titrate PFA waveforms to ablate cardiac muscle whilst sparing oesophageal smooth muscle.
Promisingly, registry data is yet to publish an oesophageal fistula caused by PFA.
Importantly, however, repeated PFA applications can result in a thermal effect, because PFA emits large currents of energy through tissue, generating resistive heating.
PFA actually emits larger voltages than RF energy, however, it pulses for a drastically reduced duration, resulting in less thermal heating. However, stacking PFA lesions in rapid succession over the same area can result in a thermal effect. Anecdotally, some labs have identified oesophageal heating with PFA when using temperature probes with un-insulated metallic electrodes. However, it is unclear if PFA is actually heating the oesophagus, or simply “inducing current flow” in the temperature probe which is being interpreted by the probes software as “heating”.
My Two Cents:
There’s rarely such a thing as “free lunch”. Ablation has some risk. Minimising ablation on the posterior wall in contact with the oesophagus seems to be a sensible strategy from a safety point of view, irrespective of ablation modality.
Whilst PFA does not yet have a published oesophageal fistula complication, temperature rises have been observed and haemolysis risk increases with increasing PFA applications.
Oesophageal fistula has a delayed presentation after discharge, most commonly presenting with fever, stroke or hematemesis 2-4 weeks after AF ablation.
This complication may have catastrophic consequences, more often than not resulting in death or stroke, irrespective of the management strategy employed.
It’s thankfully an incredibly rare complication, but this makes it difficult to quantify risk across different ablation technologies in a randomised controlled trial. However, PFA appears conceptually promising in mitigating risk of oesophageal injury.
Thanks for tuning in :)
Cheers
Mitch & CPP Team
Han HC, Ha FJ, Sanders P, Spencer R, Teh AW, O’Donnell D, Farouque O, Lim HS. Atrioesophageal Fistula: Clinical Presentation, Procedural Characteristics, Diagnostic Investigations, and Treatment Outcomes. Circ Arrhythm Electrophysiol. 2017
Martinek Martin, Hassanein Said, Bencsik Gabor, Aichinger Josef, Schoefl Rainer, Bachl Andrea, Gerstl Sebastian, Nesser Hans-Joachim, Purerfellner Helmut. Acute development of gastroesophageal reflux after radiofrequency catheter ablation of atrial fibrillation. Heart Rhythm. 2009 Oct;6 (10):1457–62
Ho SY, Cabrera JA, Sanchez-Quintana D. Left atrial anatomy revisited. Circ Arrhythm Electrophysiol. 2012 Feb;5(1):220-8.