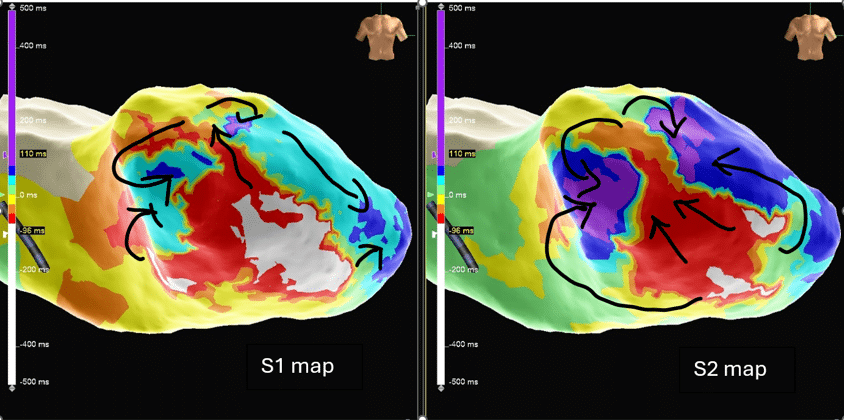
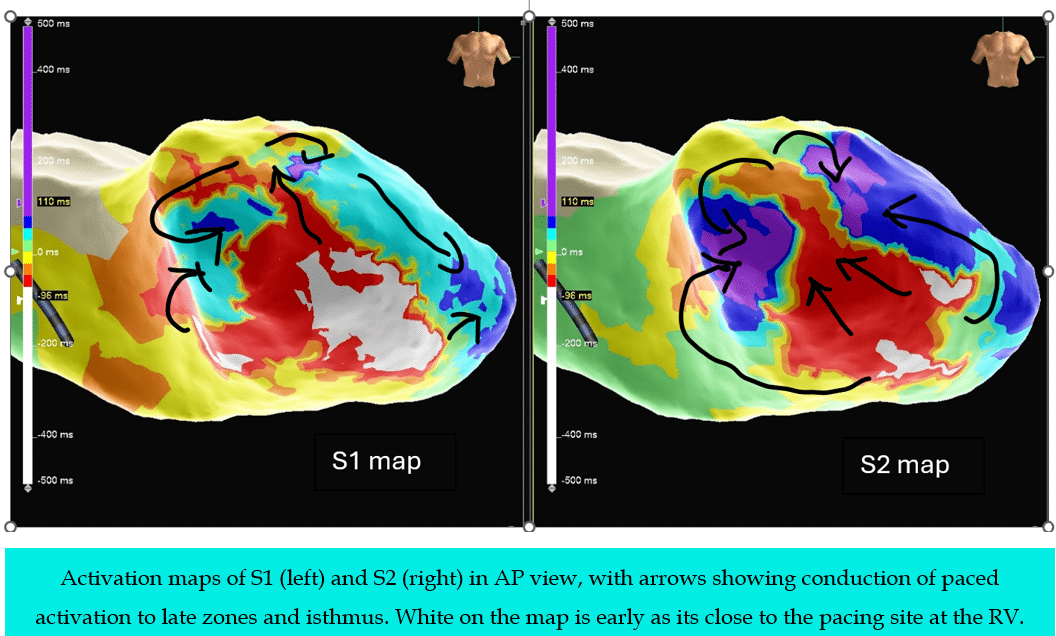
Answer: One was mapped during S1 (Drive train), the other was mapped during S2 (Extra Stimulus)
Regards
This post, including the images & videos was authored by:
Liang Shufen CEPS, CCDS
Principal Cardiac Physiologist
IBHRE Ambassador
National Heart Centre Singapore