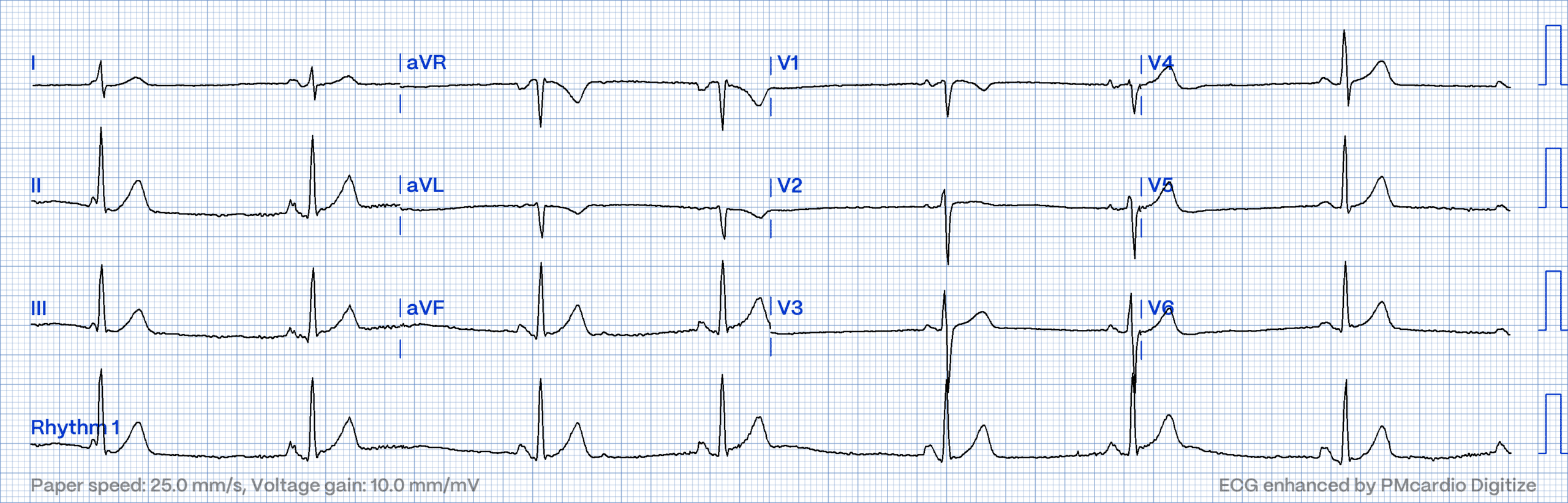
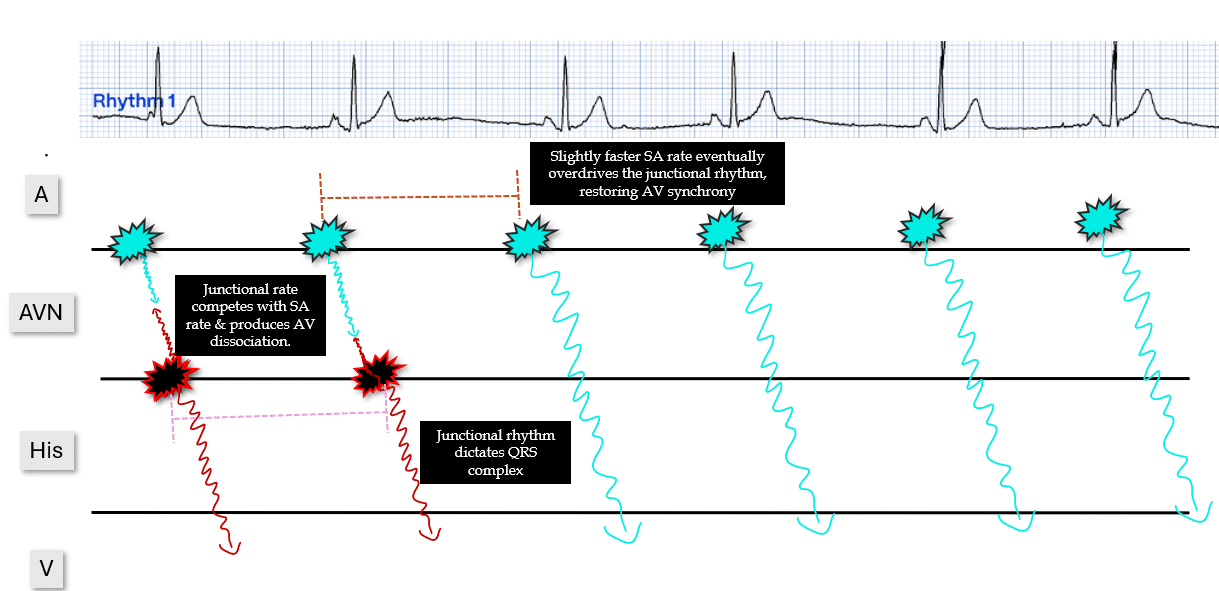
Answer: Isorhythmic AV dissociation. Generally benign, self-limiting & not cause for concern.
My Two Cents:
Thanks for tuning in :)
Cheers
Mitch & CPP Team
Learn more about the ECG features & Clinical implications of bradyarrhythmias in our ECG course here