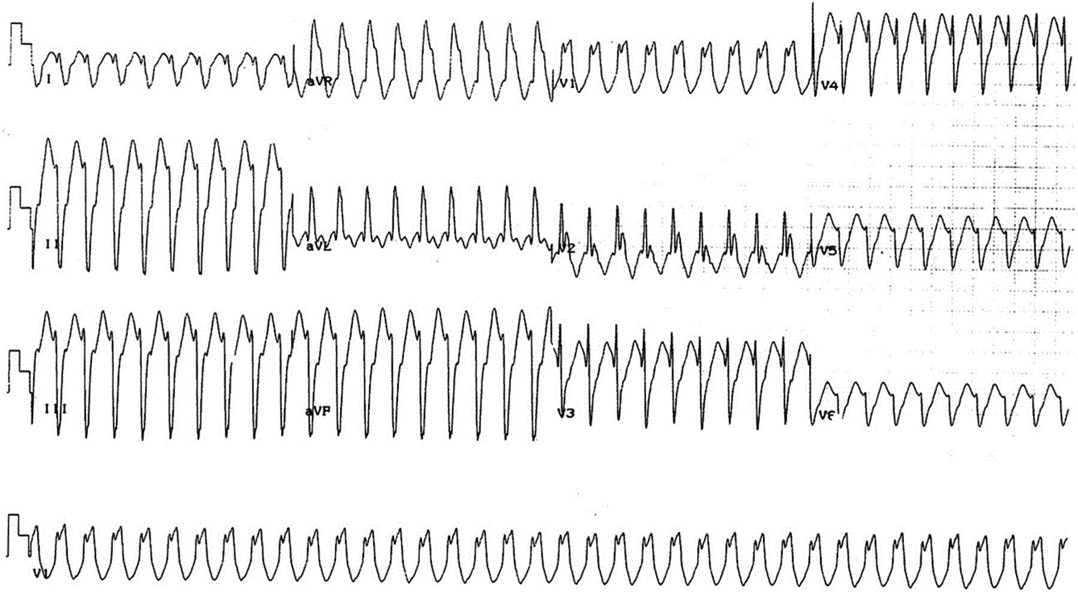
Answer: Inferoapical Left Ventricle (not far from Posteromedial Papillary Muscle)
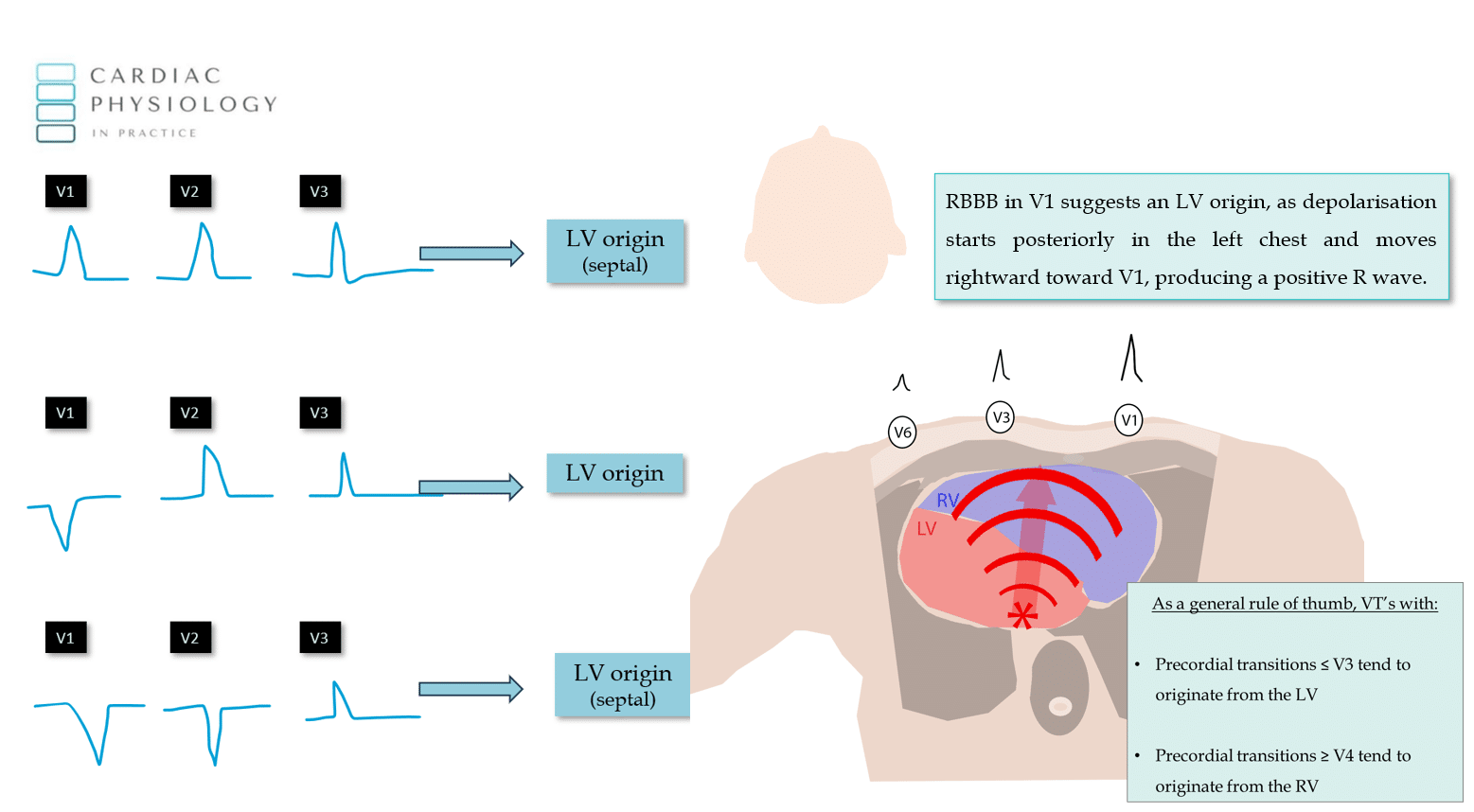
“If V1 is positive, you can bet your house its originating from the LV”
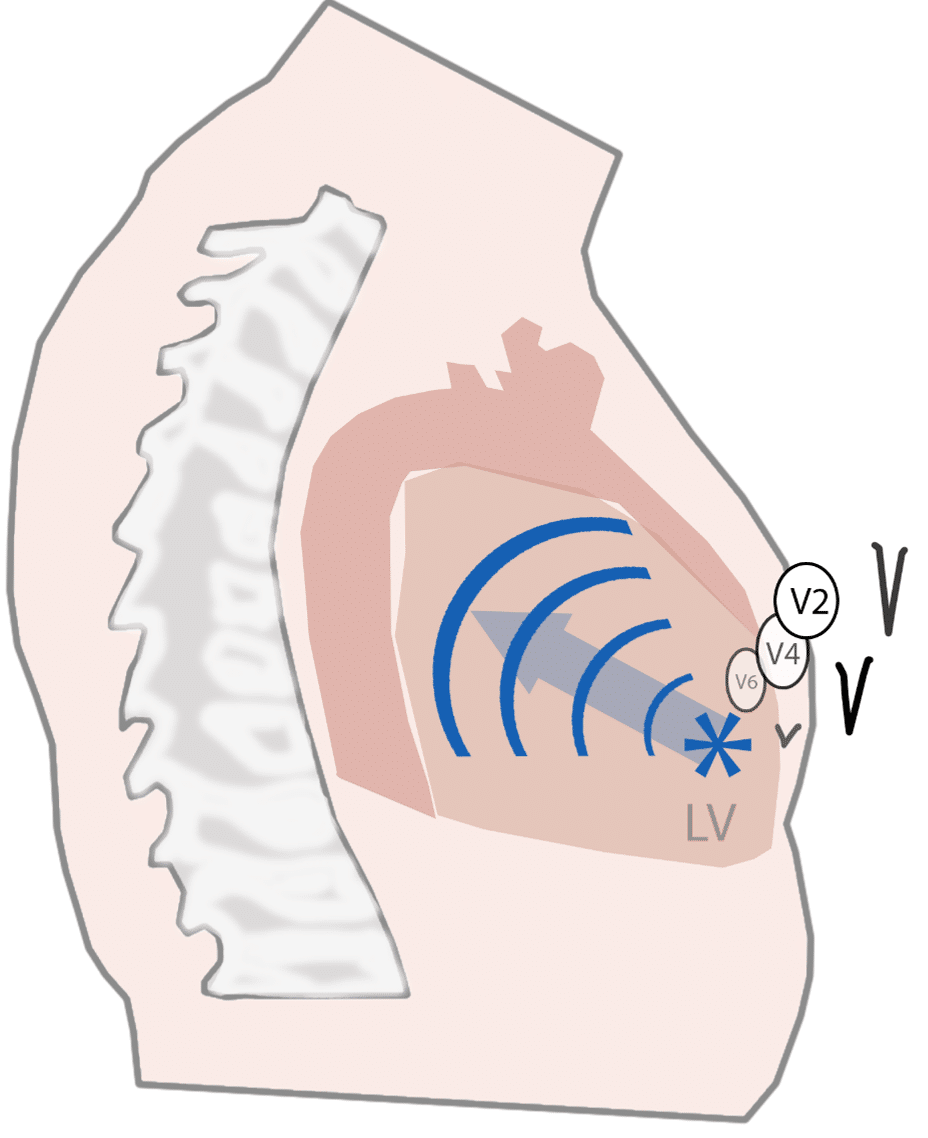
“If V2 is the first dominantly positive QRS, then you can bet your car on an LV origin”
“If V3 is the first dominantly positive QRS, then…don’t bet anything you care about, but, gun to your head with no other information, bet on the LV”
Another interesting point, is that we can surmise that this VT originates from the endocardium, and not the epicardium. This is important, because it may mean it can be treated with ablation & can give clues about the aetiology of the VT since some diseases/cardiomyopathies have propoensities for generating epicardial vs endocardial VT’s.
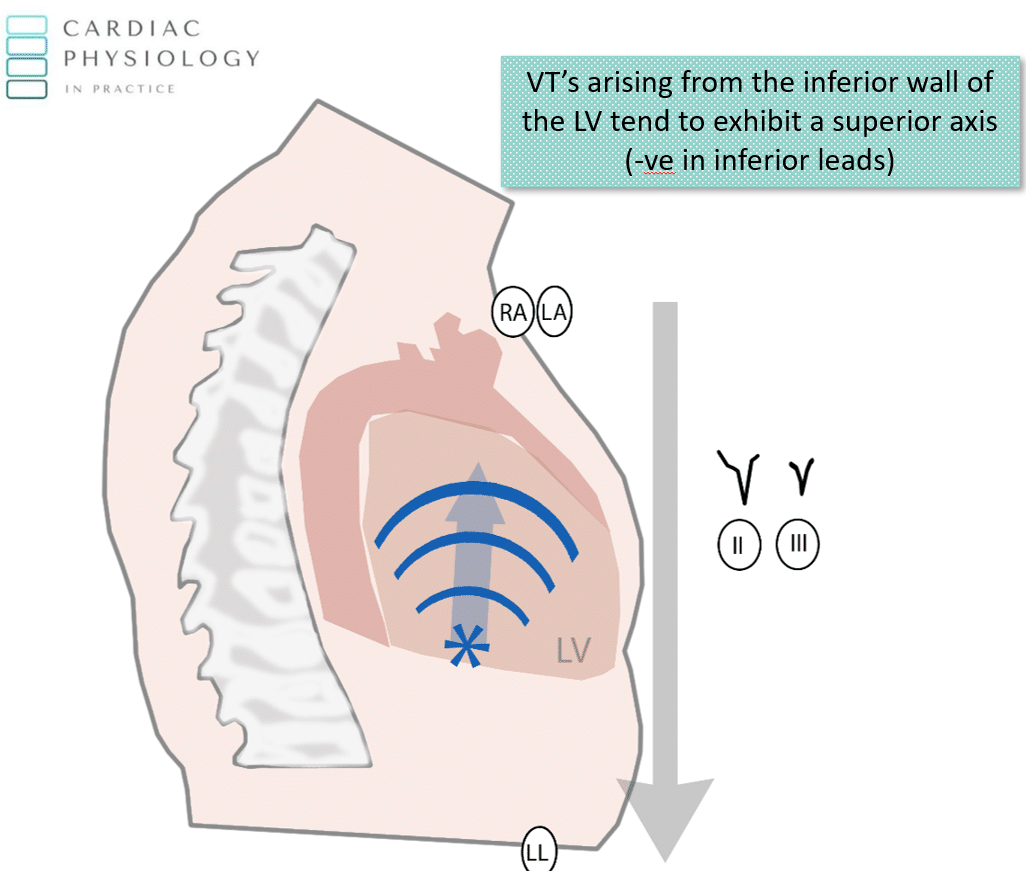
The small “r” wave in the inerior leads can be observed due to initial endocardial to epicardial depolarisation. This transmural conduction moves downwards, producing a small r wave in the inferior leads in VT’s arising from the inferior wall endocardium.
My Two Cents
Thanks for tuning in :)
Cheers
Mitch & CPP Team