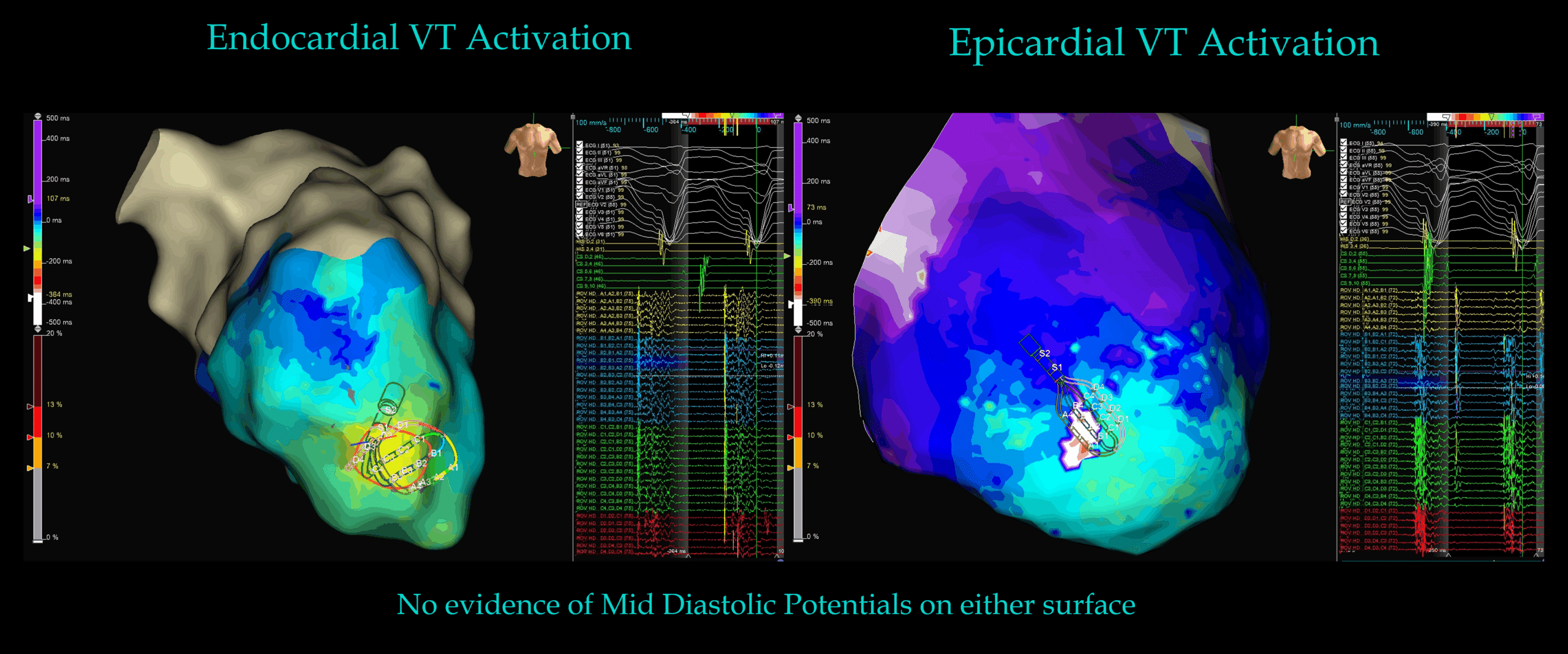
Answer: The mapped sites represented breakout rather than the critical isthmus. Critical isthmus site must be intramural, rather than endo/epicardial.



Ablation targeted both endocardial and epicardial breakout regions, resulting in non-inducibility.

My Two Cents:
Thanks for tuning in :)
Regards
Author: Dr Juan. Ismael Almonte G. (MD) with colleagues Dr Rodolfo San Antonio Dharandas (MD) and Judit Mas, Biomedical Engineer – Abbott / EnSite X Specialist.
Edited by Mitch & CPiP Team with permission.
EP in Practice – Product Overview