A patient with no structural heart disease presented with recurrent idiopathic ventricular tachycardia. During RVOT ablation, the VT morphology shifted without a change in TCL. Subsequent activation map is shown below? What anatomical structure in the RVOT can account for this change in VT morphology & exit site?
(Click to zoom on image)
Answer:
Click to Show Answer
Answer: The parietal band – part of the supraventricular crest in the RVOT.
The Case Study:
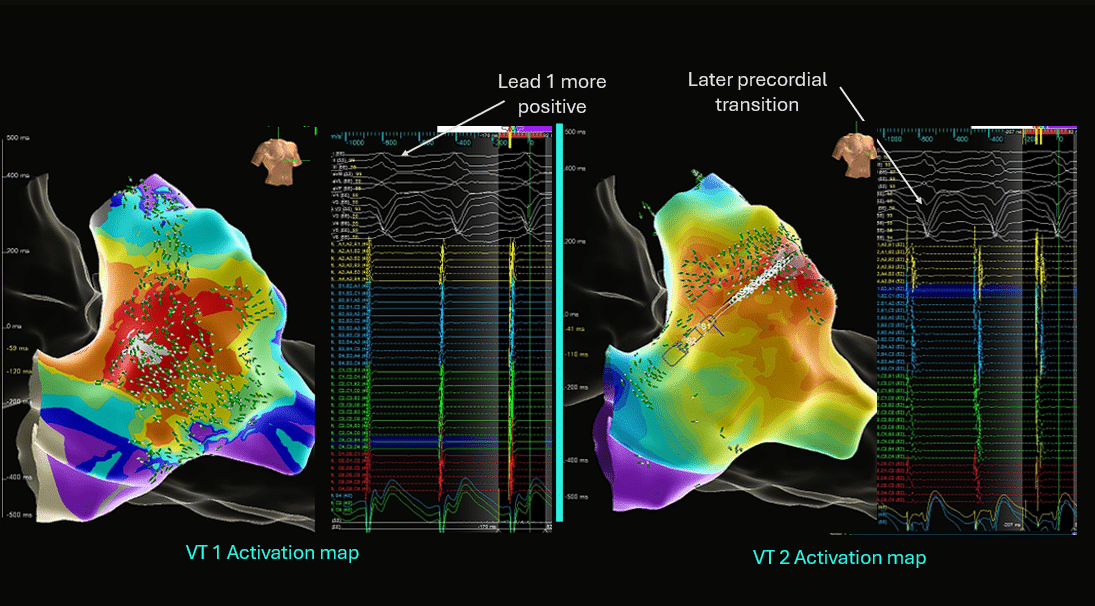
VT One
The initial VT demonstrated a typical RVOT VT morphology with two interesting features in the inferior leads:
Initial R wave slurring
Perhaps representative of initial SLOW anisotropic exit from the Parietal band due to an abrupt change in muscular fibre orientation as the VT exits the Parietal band into the RVOT.
A distinctly Notched QRS
Also described as common in Parietal band exit VT’s
Activation mapping demonstrated a focal exit site with a QS unipolar morphology in the superior-anterolateral RVOT, with a bipolar EGM preceding QRS onset by 30ms.
The change to VT2
Following ablation at this site, VT did not terminate but continued at the same TCL with a subtly DIFFERENT QRS morphology.
Repeat activation mapping demonstrated a focal exit a short distance from the initial target, along the expected trajectory of the Parietal band. EGM preceded QRS by 30ms, ablation at this site terminated VT.
Learning Points:
A change in QRS morphology during ablation may suggest multifocal RVOT arrhythmia. However, several findings argued against this interpretation:
Stable cycle length
Similar activation prematurity at both sites
Persistent focal electrogram characteristics with QS unipolar morphology
Alignment of earliest activation sites along a defined muscular structure\
These features support shifting breakout from a single intramyocardial origin rather than multiple independent foci.
The Parietal Band
The anatomical distribution of activation sites corresponded to the expected course of the right ventricular parietal band in this case.
Where is it?
Complex thick muscular structure which forms the roof of the RVOT if your are looking up form the RV apex. It extends from the septum toward the anterior wall, forming the anteroseptal border of the RVOT below the level of the pulmonary valve.
Arrhythmias from this structure aren’t particularly common, but are well described. Variable QRS morphology after initial ablation lesions due to preferential conduction within this thick muscular structure have been reported, however many case reports report initial R wave slurring and notching.
In this case, the sequential activation maps provide procedural evidence of this mechanism.
My Two Cents: Anatomical Difficulties:
Parietal Band VT’s often display initial R wave slurring & Notching in the inferior leads due to slow anisotropic exit from the Parietal band.
Ablation of VT arising from the Parietal band can result in changes in Exit sites, leading to the operator chasing VT exit sites – they often require more ablation.
Catheter contact & stability can be challenging along this ridge, depending on the angle of catheter, frustrating mapping & ablation attempts.
The band can be thicker than the surrounding myocardium. Too little ablation along the Parietal band can result in inadequate lesion depth.
However, what if the Operator has slid off the Parietal band and has their catheter in contact with the surrounding thin RVOT wall? Too much ablation here risks injury & perforation. This can make ablation of arrhythmias in this location challenging.
It’s important to appreciate the anatomy of the RVOT to optimise safety & efficacy.
Thanks for tuning in :)
Regards
Primary Author: Dr Juan. Ismael Almonte G. (MD)
with colleagues Dr Rodolfo San Antonio Dharandas MD, Dr Alfredo Chauca MD, & Judit Mas (Bioengineer).
Yamada T, Yoshida N, Itoh T, Litovsky SH, Doppalapudi H, McElderry HT, Kay GN. Idiopathic Ventricular Arrhythmias Originating From the Parietal Band: Electrocardiographic and Electrophysiological Characteristics and Outcome of Catheter Ablation. Circ Arrhythm Electrophysiol. 2017 Aug;10(8):e005099. doi: 10.1161/CIRCEP.117.005099. PMID: 28794085.
Ho, Siew & Hosseinpour, Amir-Reza. (2021). Supraventricular crest: Structure, function and implications for surgical resection in tetralogy of Fallot. International Journal of Cardiology Congenital Heart Disease. 4. 100112. 10.1016/j.ijcchd.2021.100112.