
TLDR: The P wave morphology is consistent with a right superior posterolateral origin of atrial depoalrisation, which is consistent with the location of the SA Node.
The complexity of the Sinus Node Anatomy was discussed in the previous beatbox. It’s generally considered a “posterolateral” structure at the SVC/RA junction. This means that the P wave morphology which it generates, is generally consistent with:
1. A Right atrial structure
2. A Superior structure
3. A Right Lateral structure
4. A Posterior structure
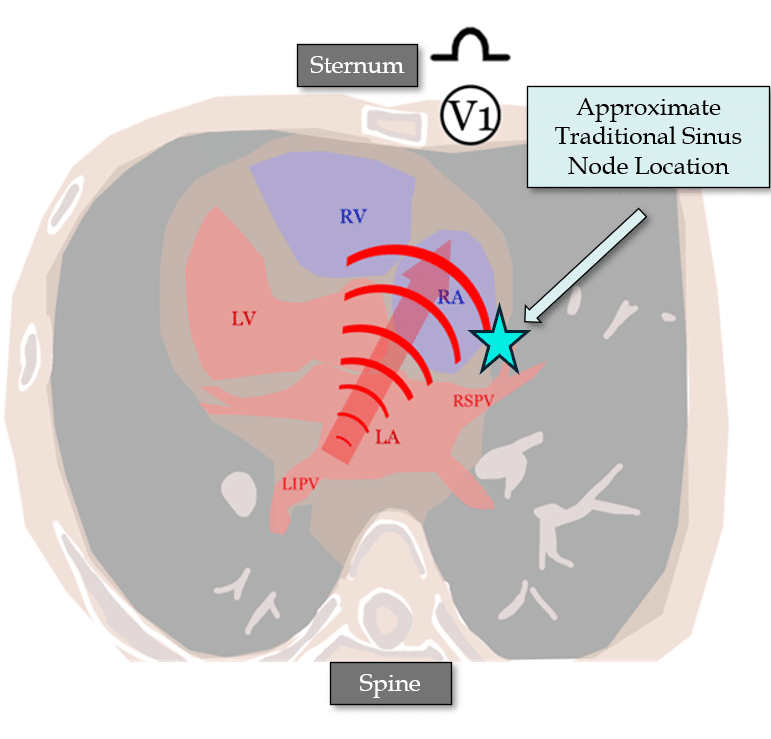
As we discussed last Beat Box, this can change, depending on whether the so-called “head” or “tail” of the sinus node is dominant, and where the depolarisation exits the epicardium and enters the endocardium.
Lets look at how we can localise the Sinus Location, using the 12-lead P wave morphology.
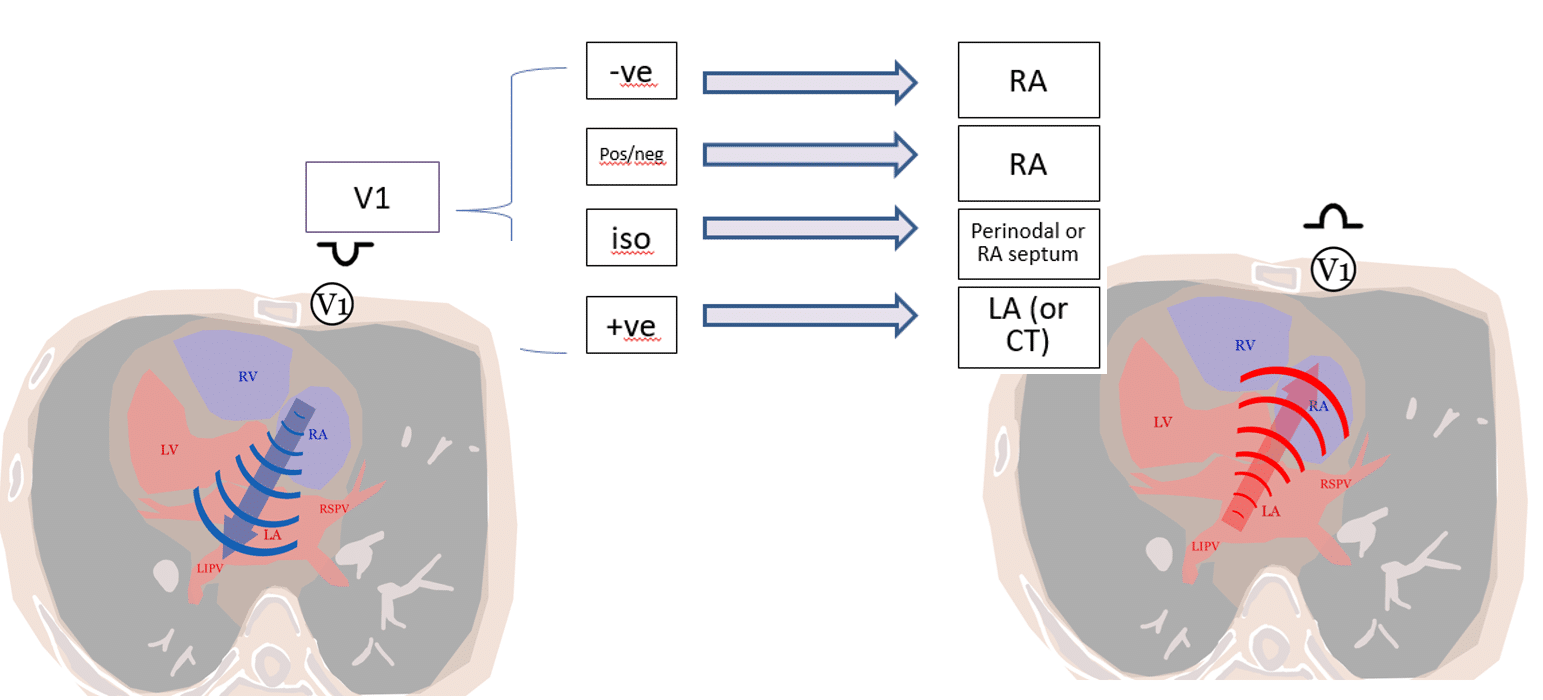
To determine this, we analyze V1:
A wavefront moving towards V1 produces a positive P wave, while one moving away from V1 produces a negative P wave.
Sinus P waves are classically biphasic (Pos/Neg) in V1 because:
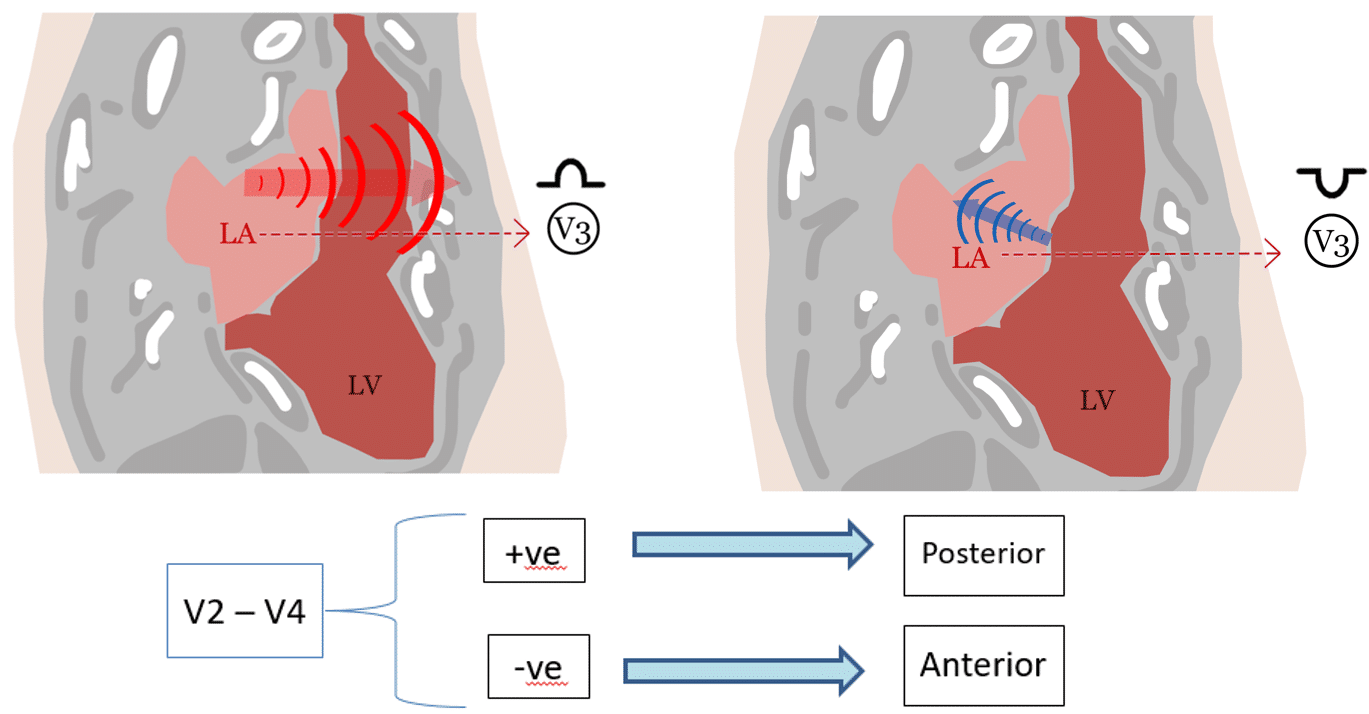
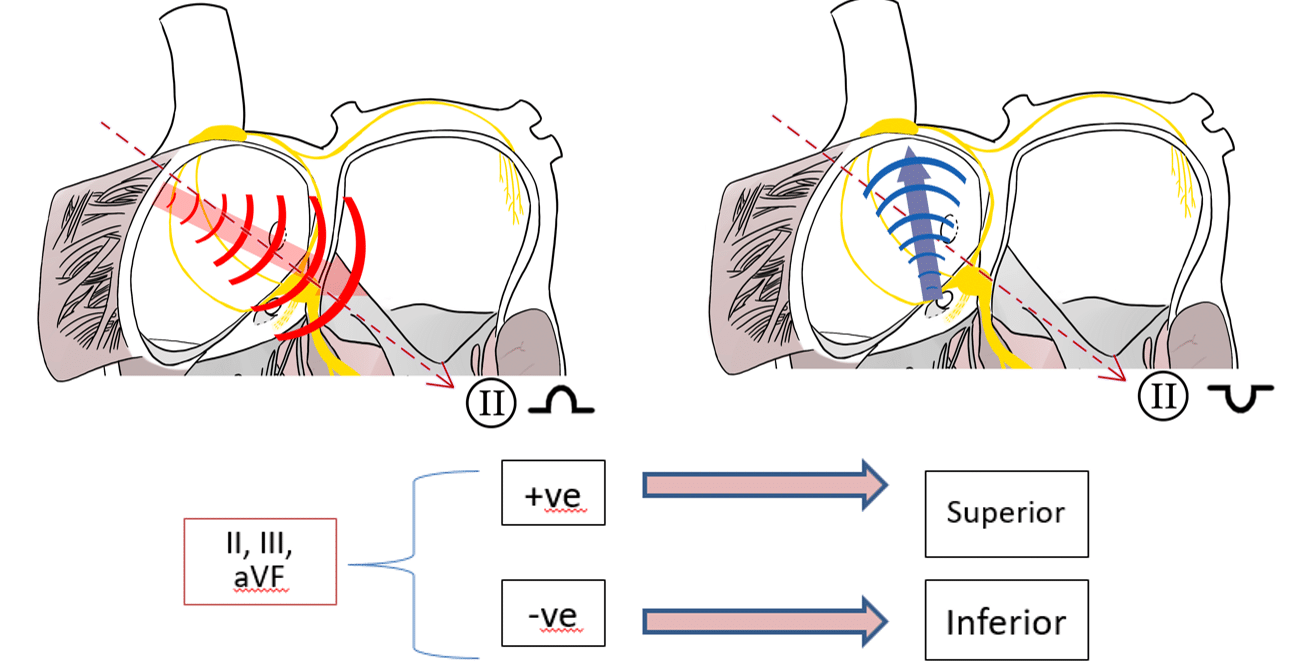
The diagrams below summarises how different atrial arrhythmia origins origins produce different P wave morphologies.
My two cents: So now, we’ve described what a sinus p wave looks like:
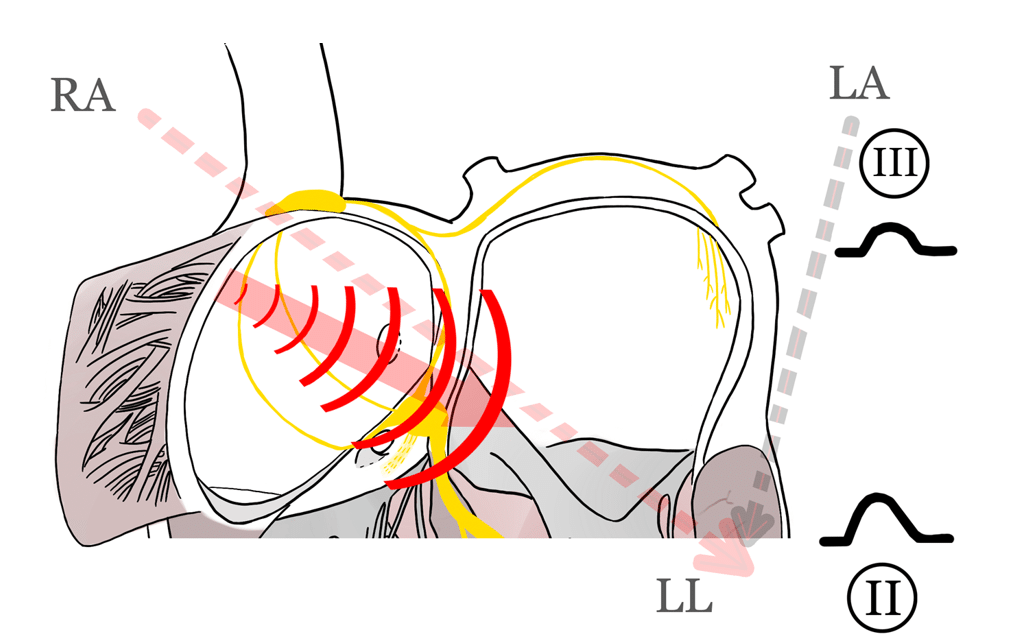
Bonus tip = lead II is more positive than lead III, since the SA node is a right lateral structure.
We will revisit these P wave localisation principles when we dive into Focal AT ECG’s in future BeatBox posts. For those who want to read ahead, the below references are the seminal papers on P wave localisation.
Thanks for tuning in :)
Cheers
Mitch & CPiP Team.
References & Seminal papers on this subject:
Kistler PM, Chieng D, Tonchev IR, Sugumar H, Voskoboinik A, Schwartz LA, McLellan AJ, Prabhu S, Ling LH, Al-Kaisey A, Parameswaran R, Anderson RD, Lee G, Kalman JM. P-Wave Morphology in Focal Atrial Tachycardia: An Updated Algorithm to Predict Site of Origin. JACC Clin Electrophysiol. 2021 Dec;7(12):1547-1556.
Kistler PM, Roberts-Thomson KC, Haqqani HM, Fynn SP, Singarayar S, Vohra JK, Morton JB, Sparks PB, Kalman JM. P-wave morphology in focal atrial tachycardia: development of an algorithm to predict the anatomic site of origin. J Am Coll Cardiol. 2006 Sep 5;48(5):1010-7.