Answer:
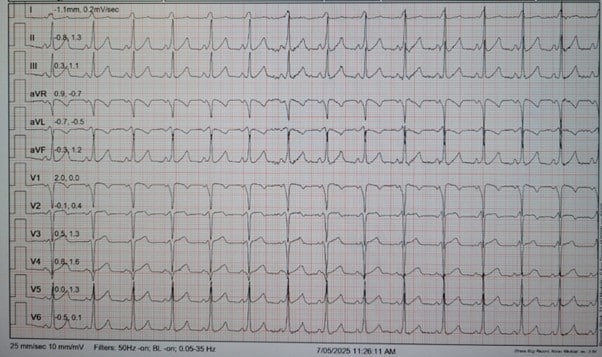
The baseline ECG shows:
Suggestive of the presence of an accessory pathway.
Now, to take ECG interpretation to the next level is to localise it to optimise ablation. If you pay a little more attention to the delta wave pattern, QRS transition, and axis, you can predict the likely location of the accessory pathway before the patient even hits the EP lab.
In WPW, the delta wave tells you where the ventricle is being activated early.
From there, it is possible to work backwards to find the atrial–ventricular connection.
This allows us to narrow down the likely insertion site, optimise the first mapping site and vascular approach & avoid “wandering” with the catheter, reducing time, radiation, and risk.
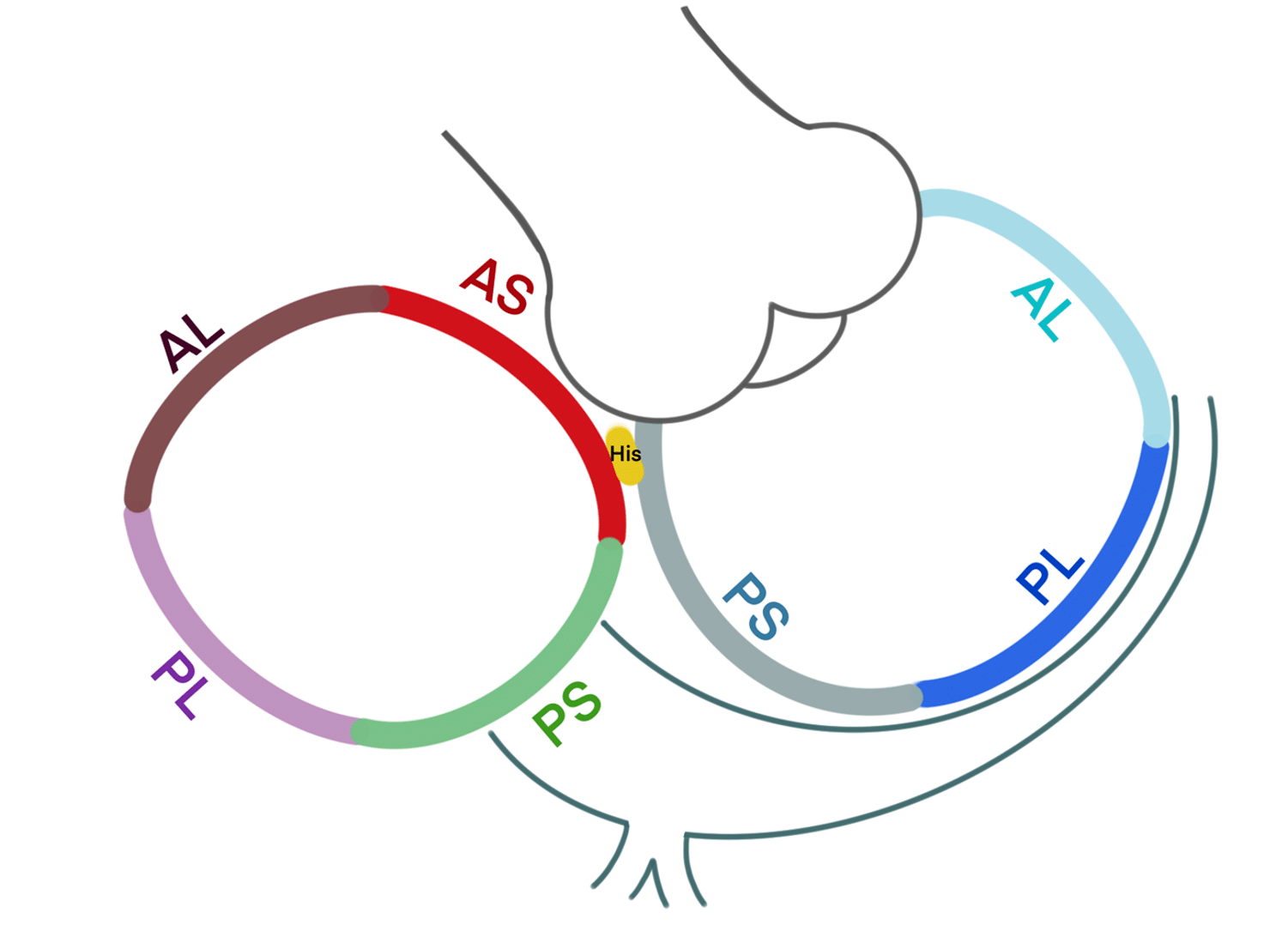
Accessory pathways are classified by annular position — left free wall, right free wall, or septal (anteroseptal, midseptal, posteroseptal).
Core ECG clues:
| Lead group | What to look for | What it suggests |
| Lead I / aVL | Delta wave polarity | Positive in I/aVL → right-sided AP; Negative → left-sided AP |
| Lead V1 | Delta polarity & QRS transition | Positive delta in V1 → left-sided; Negative delta in V1 → right-sided |
| QRS Transition (precordial) | Earliest positive R wave | Early transition (V1–V2) → left sided; |
| Axis | QRS axis shift | Superior axis (negative in II, III, aVF) → Posterior AP; Inferior axis (positive in II, III, aVF) → Anterior AP |
For example:
It informs patient discussion, consent and procedural strategy.
| Feature | Observation | Interpretation |
| Lead I / aVL | Positive delta (aVL is challenging, I think still positive for the initia’ “delta wave”. | Right-sided |
| Lead V1 | Negative delta | Right-sided |
| QRS Transition | Challenging – open to interpretation, but I think V2 has an initially positive delta wave. | Indicates Right Septal |
| Axis | Inferior (positive II, III, aVF) | Anterior annular position |
Localisation Conclusion: Right Anteroseptal accessory pathway
My two cents:
Think of interpreting an ECG as using Google Maps in the EP lab. We use it to find where we need to go and skipping localisation is like setting off on a road trip without directions. When you don’t use a map, you might get to the destination eventually, but it could take longer, cost more, and you’re more likely to run into some trouble along the way.
Thanks for tuning in.
Kenny & CPiP Team
References
Arruda M, et al. J Cardiovasc Electrophysiol. 1998;9(1):2–12.
Fitzpatrick AP, et al. J Am Coll Cardiol. 1994;23(1):107–116.
Josephson ME. Clinical Cardiac Electrophysiology: Techniques and Interpretations. 5th ed. Wolters Kluwer; 2021.
Wren C, Vogel M. Europace. 2019;21(9):1409–1416.