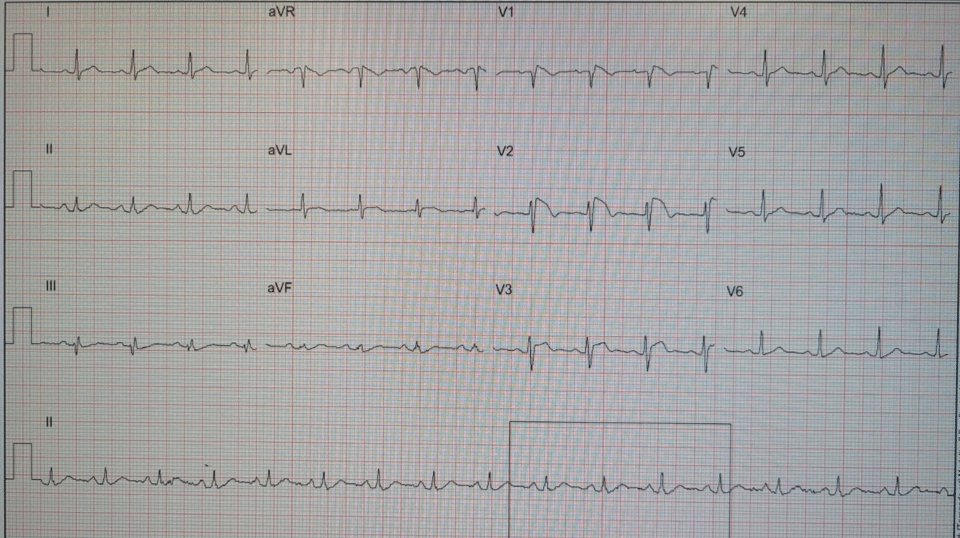
Answer: Spontaneous Type 1 Brugada ECG pattern present V1-V2 (most prominent in V2). With a history of unexplained syncope, a diagnosis of Brugada Syndrome should be considered (depending on the history/features of the syncopal event).
Brugada “ECG pattern”
Brugada “Syndrome”
Refers to someone who has:
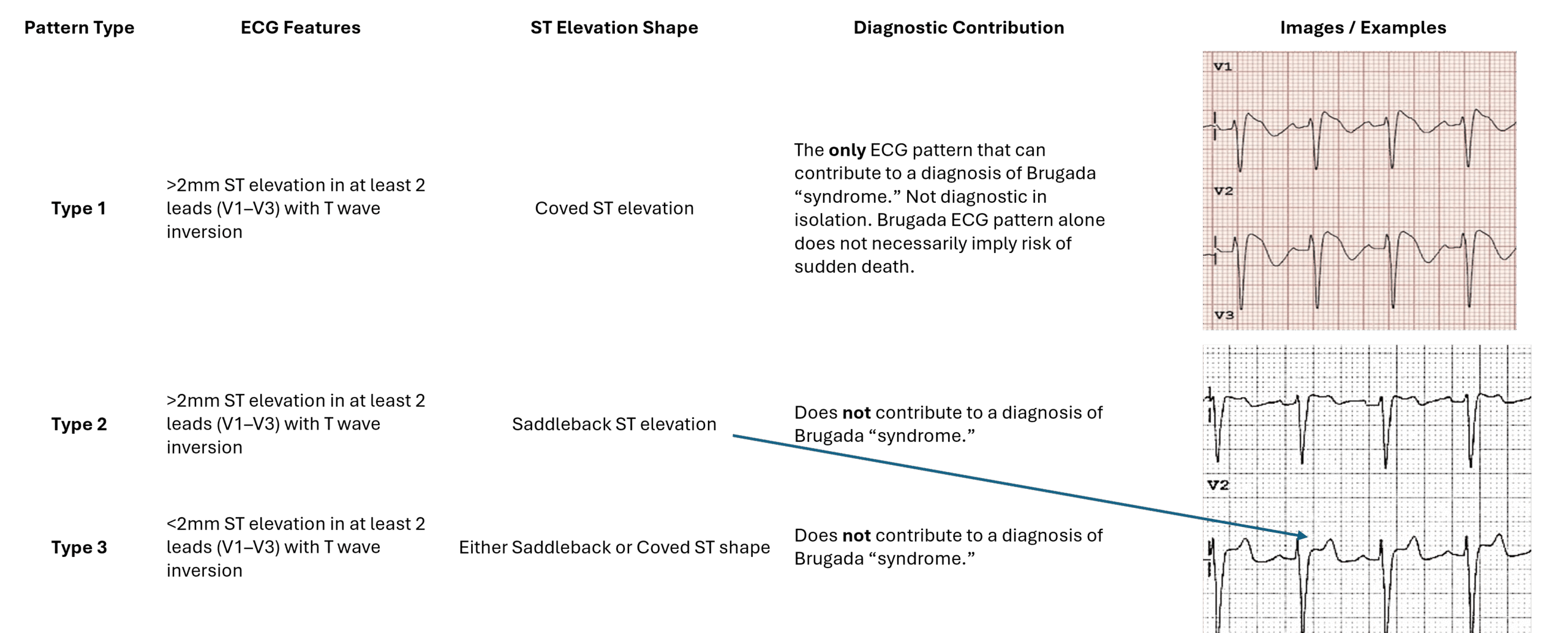
Type 2 or Type 3 Brugada ECG pattern CANNOT be Brugada syndrome unless a type 1 ECG pattern has been observed/manifested with medication.
Brugada “syndrome” is usually diagnosed in the presence of a type 1 ECG pattern & a history of symptoms, either:
Congenital channelopathy that increases a person’s risk of ventricular fibrillation.
The Brugada ECG pattern is DYNAMIC, transient and variable and can change by the hour.
Type 1 Brugada ECG pattern is more likely to occur during:

Patients with T1 Brugada ECG pattern and a history of syncope due to likely VF, or documented VT/VF are often treated with an ICD.
Entirely asymptomatic patients with an incidental Brugada pattern ECG are often managed conservatively if they lack symptoms or risk factors. An ECG alone is not usually sufficient to determine a patients risk of VF or their need for ICD therapy. More information is usually needed.
My Two Cents:
This BeatBox post was based on content contained in ECG in Practice
ECG in Practice – Product Overview
References: