
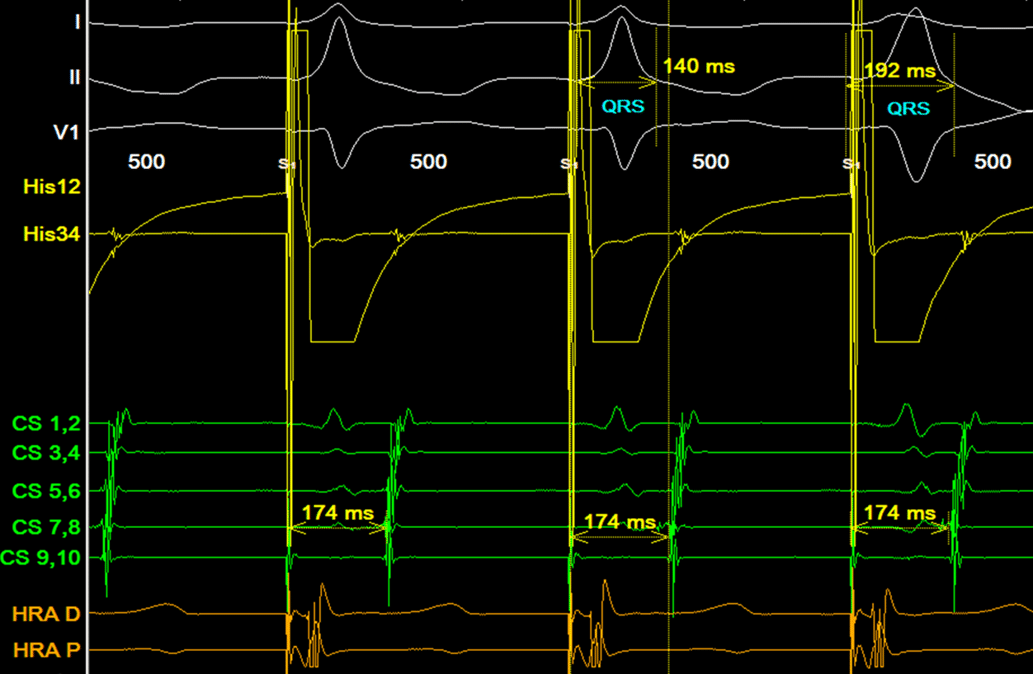
Answer: A (visually) long VA time makes slow/fast AVJRT unlikely. Spontaneous termination with the atrium as the last EGM of tachycardia makes Focal AT unlikely.

So… given the scenarios above, we can infer the following:

For the people who doubt that circled EGM is a pathway potential, here is the result of our parahisian pacing.
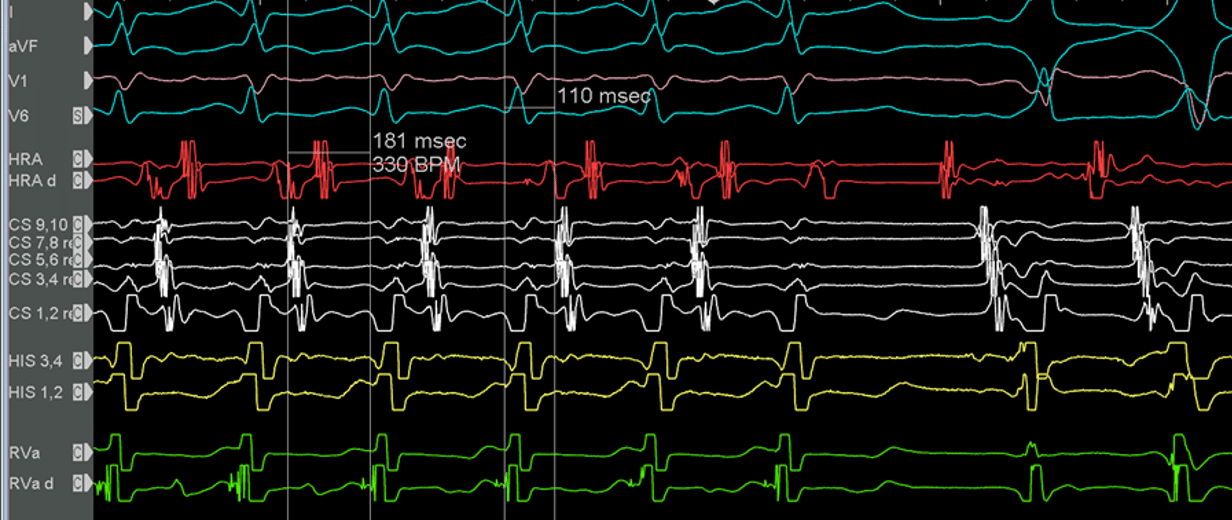
The Above EGM demonstrates a narrow complex tachycardia with a VA time of 110ms and eccentric atrial activation. This is strongly suspicious for ORT.
Termination occurs in the Ventricle in this scenario. What does this tell us?
My Two Cents:
Thanks for tuning in :)
Cheers
Mitch & CPiP Team
This post was based on a Mini-Lecture from the SVT Program of EP in Practice. No Compromises. No Shortcuts. Just EP Mastery.
EP in Practice – Product Overview