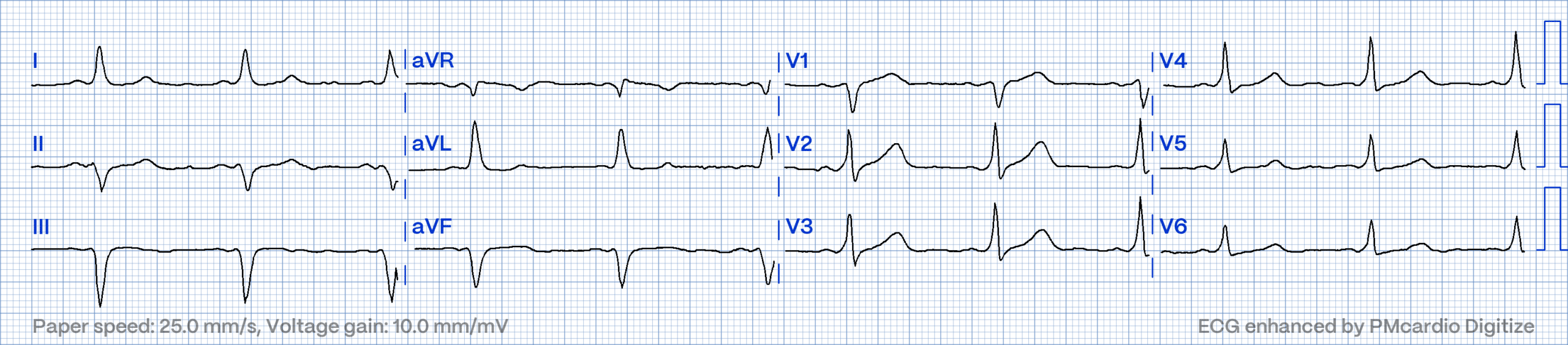
Answer: Sinus rhythm with manifest pre-excitation indicative of an antegrade conducting accessory pathway. Also known as “WPW pattern” – not syndrome.
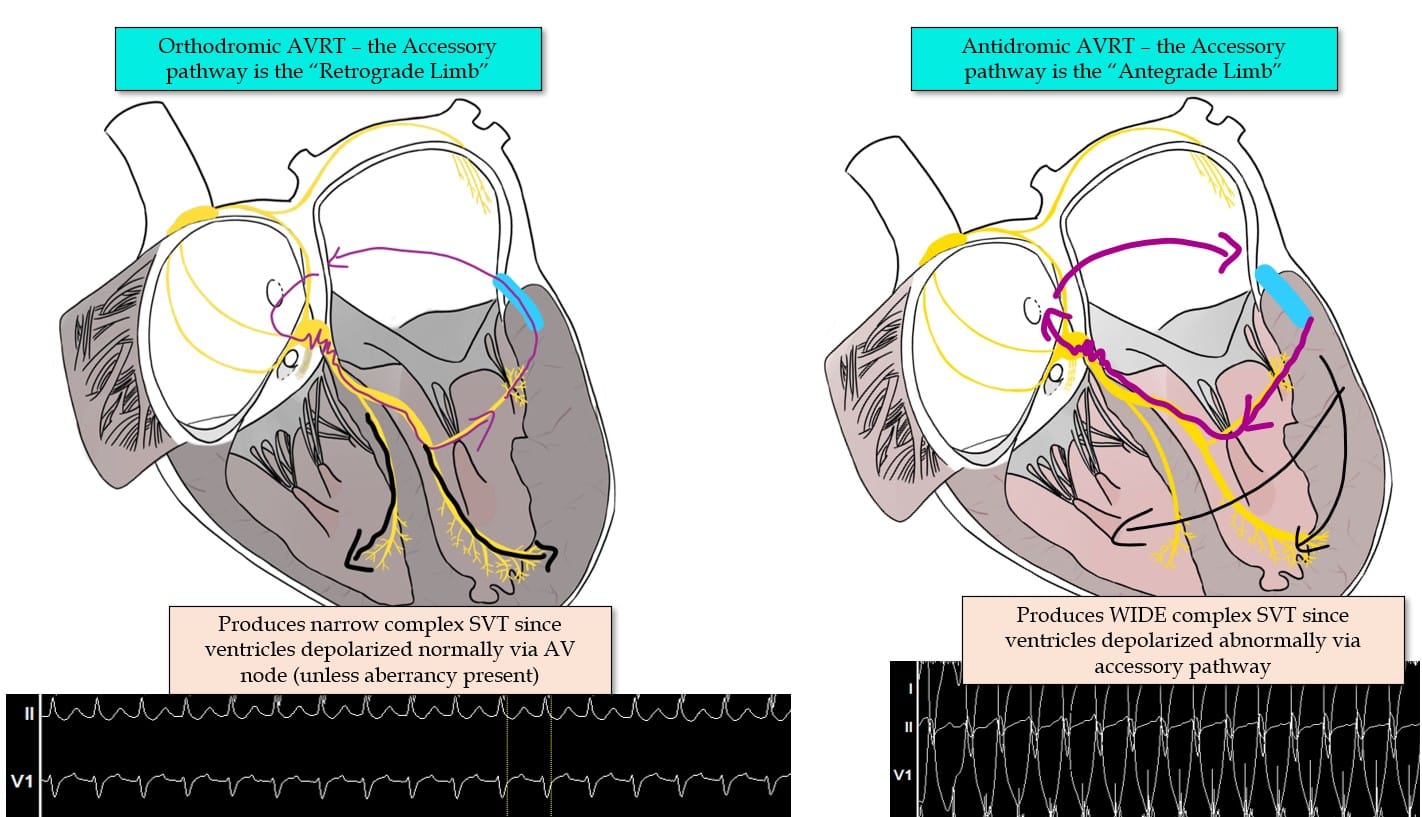
A small proportion (approx. 1 in 1000) of people born with an extra electrical connection between the Atria & Ventricles known as an “Accessory Pathway” or “Bypass Tract”. This extra electrical connection allows for a re-entrant circuit to form between the AV node and Accessory pathway, sustaining an SVT circuit. This accessory pathway can be targeted with ablation to “cure” SVT.
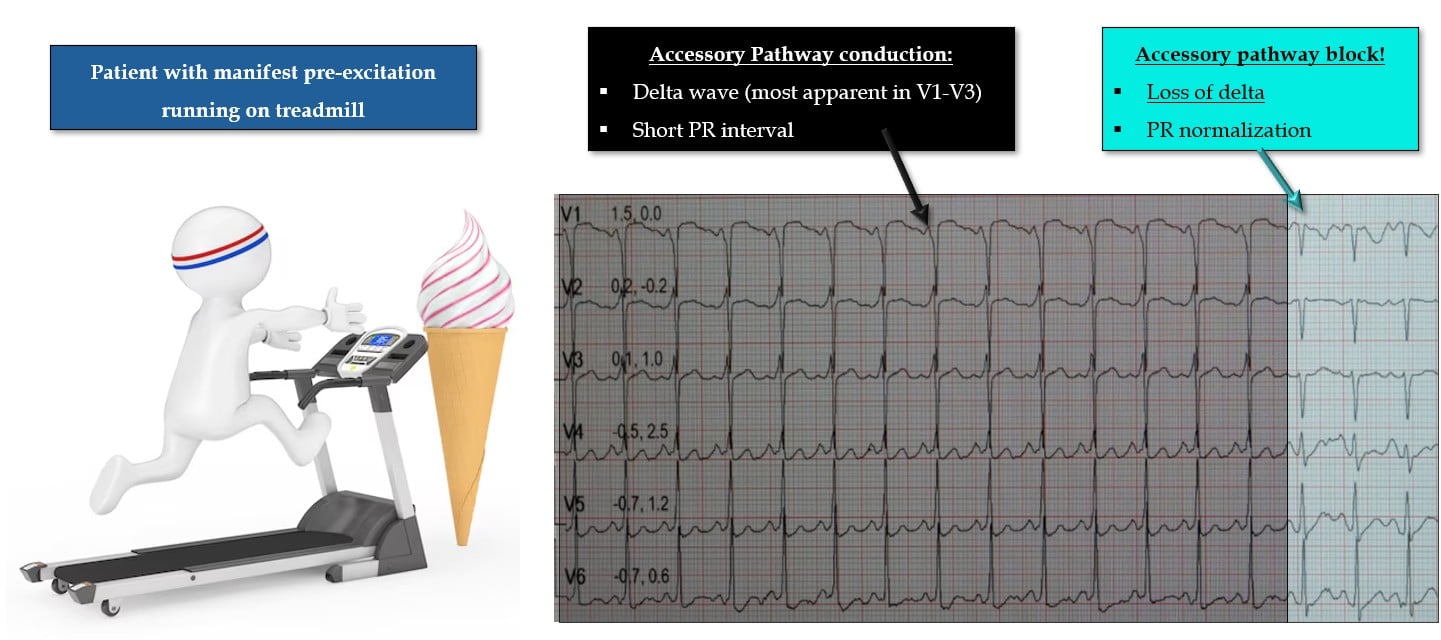
1. Short PR interval:
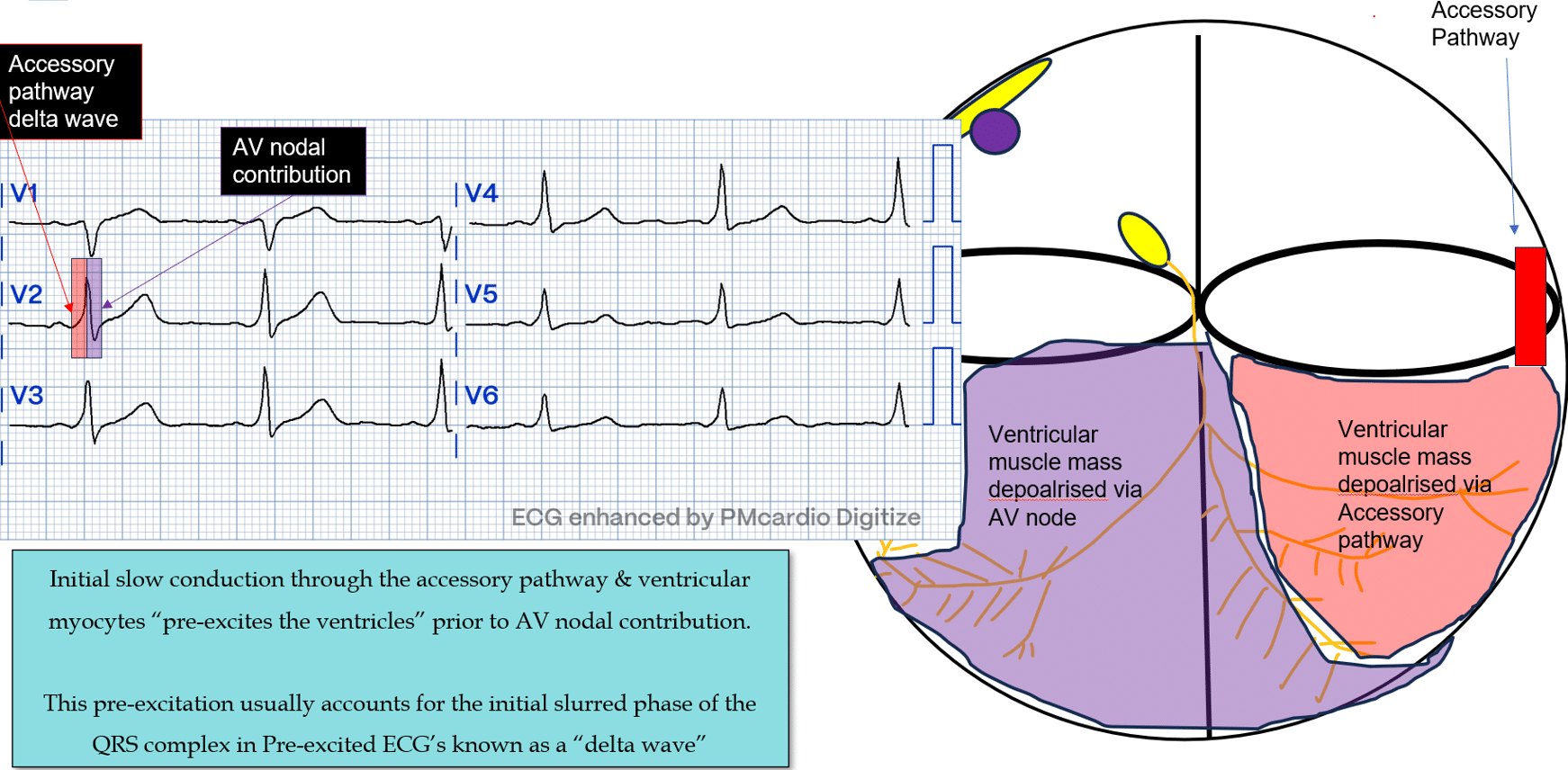
2. The Delta Wave
3. Abnormal repolarisation:
1. Many (and perhaps the majority of) accessory pathways do not conduct in an antegrade direction – they may participate in orthodromic AVRT, but do not display signs of pre-excitation on a resting ECG.
- They only way to know for sure if the patient has a retrograde-only conducting pathway is via an EP study.
2. Not all people with accessory pathways will experience an SVT episode, although the presence of an accessory pathway does predispose someone to SVT (specifically AVRT).
An asymptomatic patient such as in our scenario, therefore often does not require treatment, except for in very specific circumstances where there are occupational concerns, or concerns regarding concurrent atrial fibrillation and sudden death risks.
3. ***Important Nomenclature to know***
“Pre-excitation” & “WPW-pattern” refer to a resting ECG with signs of pre-excitation.
My Two cents:
Thanks for tuning in :)
Cheers
Mitch & the CPiP Team
Learn more by joining up to our EP course, EP in Practice. Our goal for the EP course is to be unapologetically comprehensive—even if that means it’s longer and more content-rich than other education programs. EP is also evolving rapidly, and you deserve an EP course that rapidly evolves with it. We welcome new contributors as fresh research, methods, and ideas emerge. As part of EP in Practice, you’ll also have lifetime access to all future updates.