
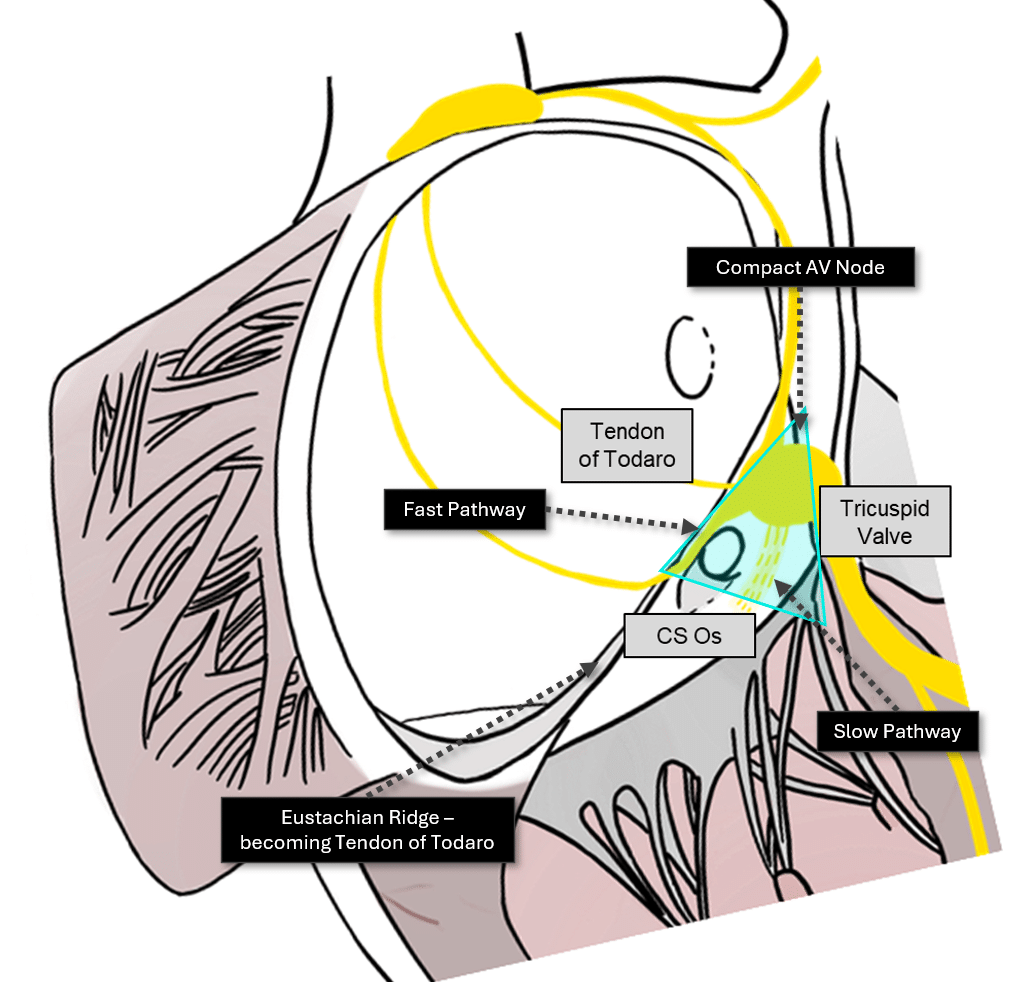
The illustration below describes the 3 sides of the triangle:
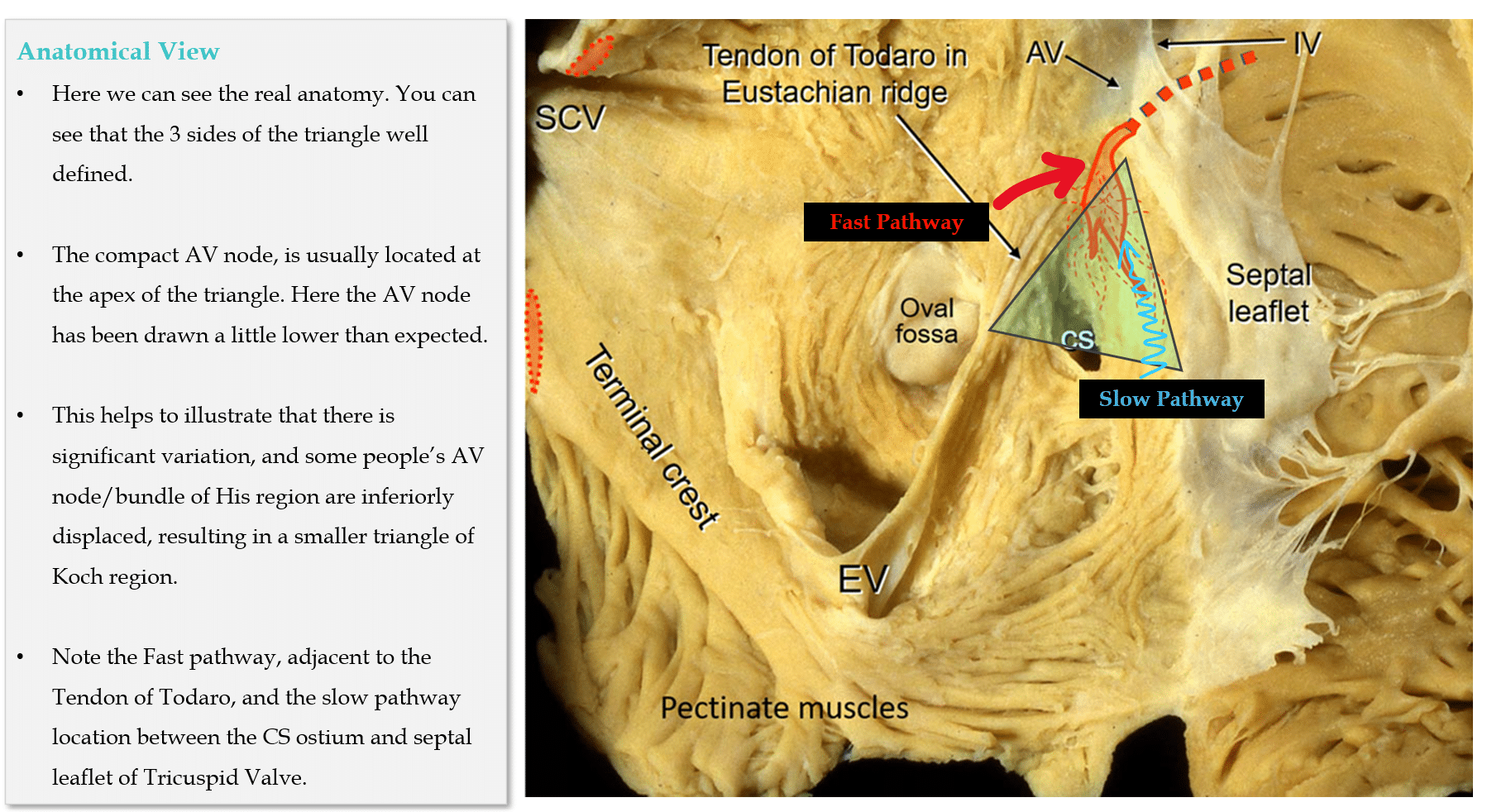
Anatomical Considerations for His Bundle Pacing. Circ Arrhythm Electrophysiol. 2019;12(7):e006897
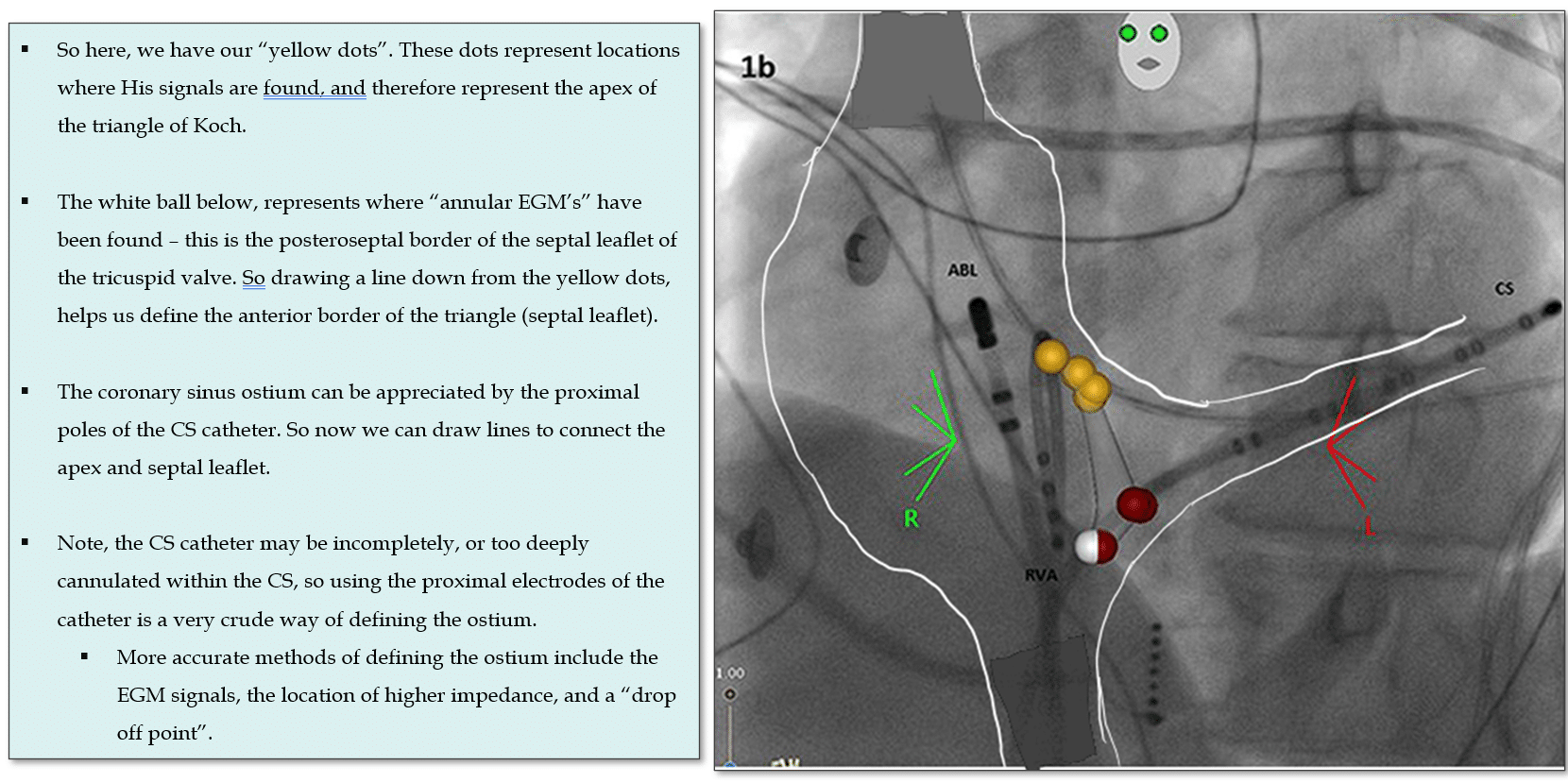
The method I’ve described is a little crude and serves as a rough guide at a glance. In reality, EGM’s are in fact the only source of truth, and the EGM’s will help to fine tune our triangle. So the “red line” or anterior border will be defined by the location we have “annular signals” and the Apex will be defined by a position just proximal to His signal EGM’s.
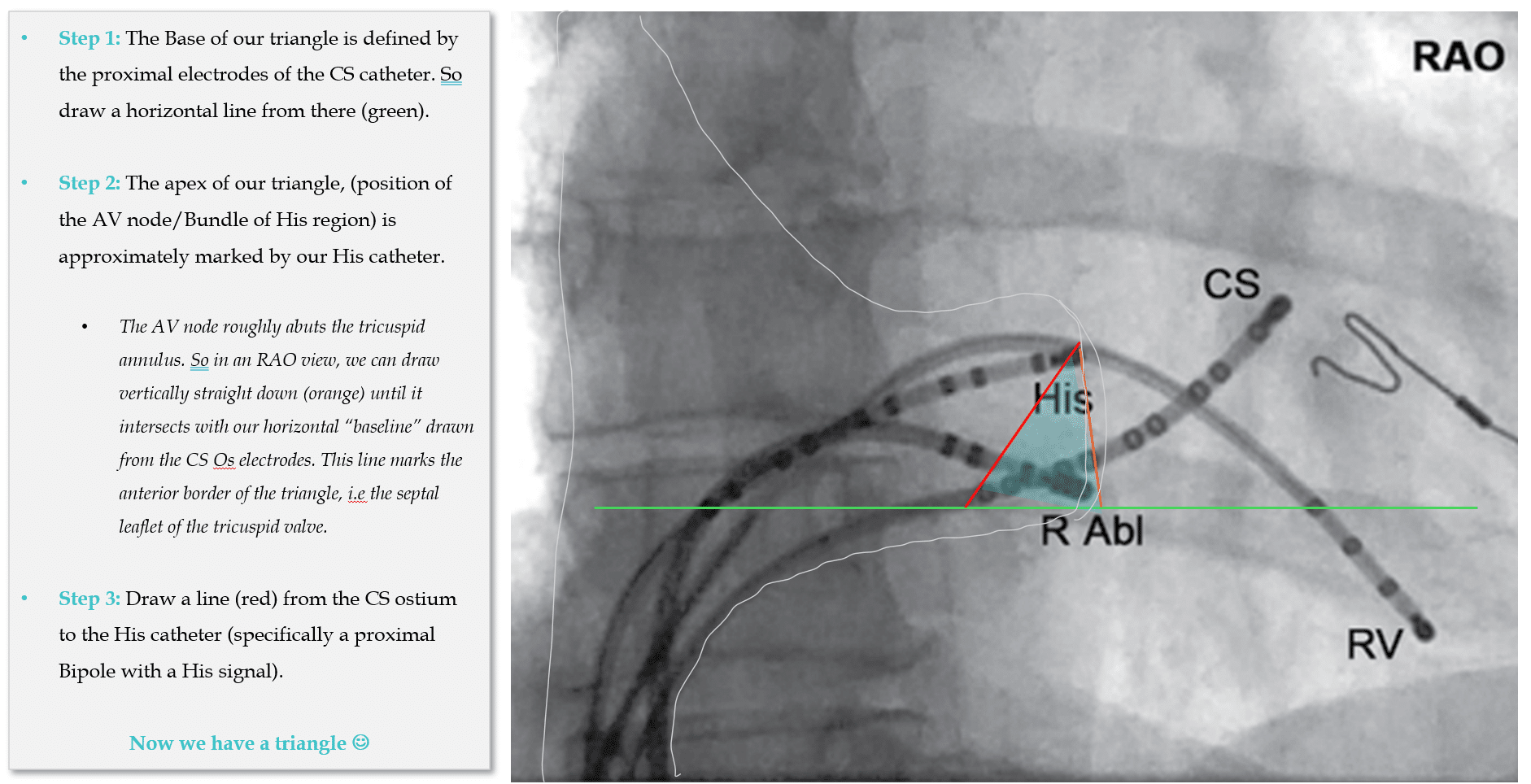
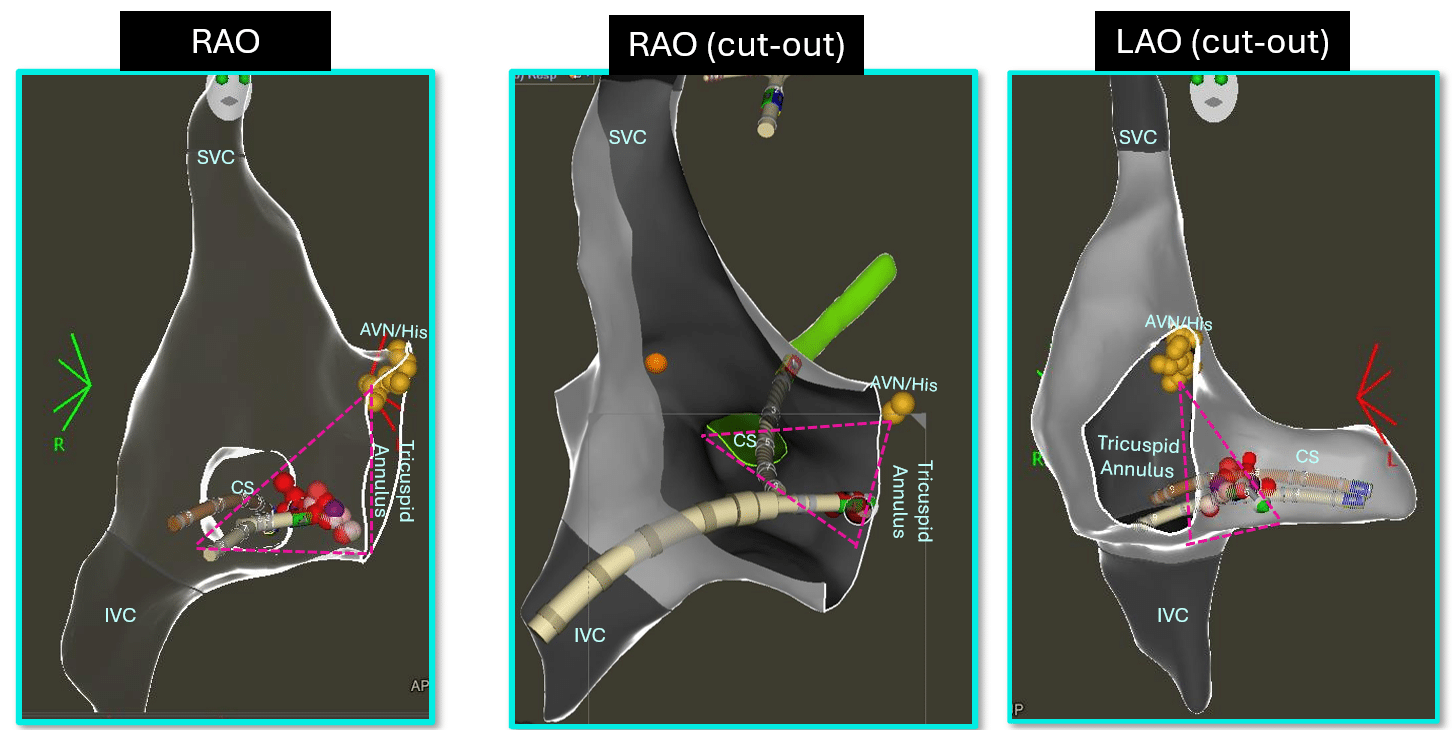
Also, neither the LAO nor the RAO view gives us a perfect view of the triangle. So lets look at an LAO view next.
So lets looks at how 3D mapping relates to a fluoroscopic view, this time in a LAO view which helps you differentiate the “lateral dimension” of the triangle. I.e “septal vs lateral”.
I have tried to draw an approximate outline of the RA over the top of this fluro image, to help you orientate yourself in the atrium -it’s not perfect, but hopefully it helps.
My Two Cents:
Thanks for tuning in :)
Cheers
Mitch & CPiP Team
References:
Nagarajan VD, Ho SY, Ernst S. Anatomical Considerations for His Bundle Pacing. Circ Arrhythm Electrophysiol. 2019 Jul;12(7):e006897.