This map & EGM set were obtained during an Atypical Flutter. Given the LAT histogram, & the Map what sort of atrial flutter is present & what ablation strategy can be used to prevent this arrhythmia?
Ablation strategy can be any of the lines shown below, connecting the mitral annulus to an electrically inert structure (usually a pulmonary vein which has been isolated).
Figure adapted from: Cho Y, et al. 2012 Aug;14(8):1104-11.
This Beat Box will focus on Posterolateral MI lines:
Usually the shortest line ablation compared to the other two possible lines.
However, tissue can be thick (though often less thick compared to Anterolateral line which is also longer).
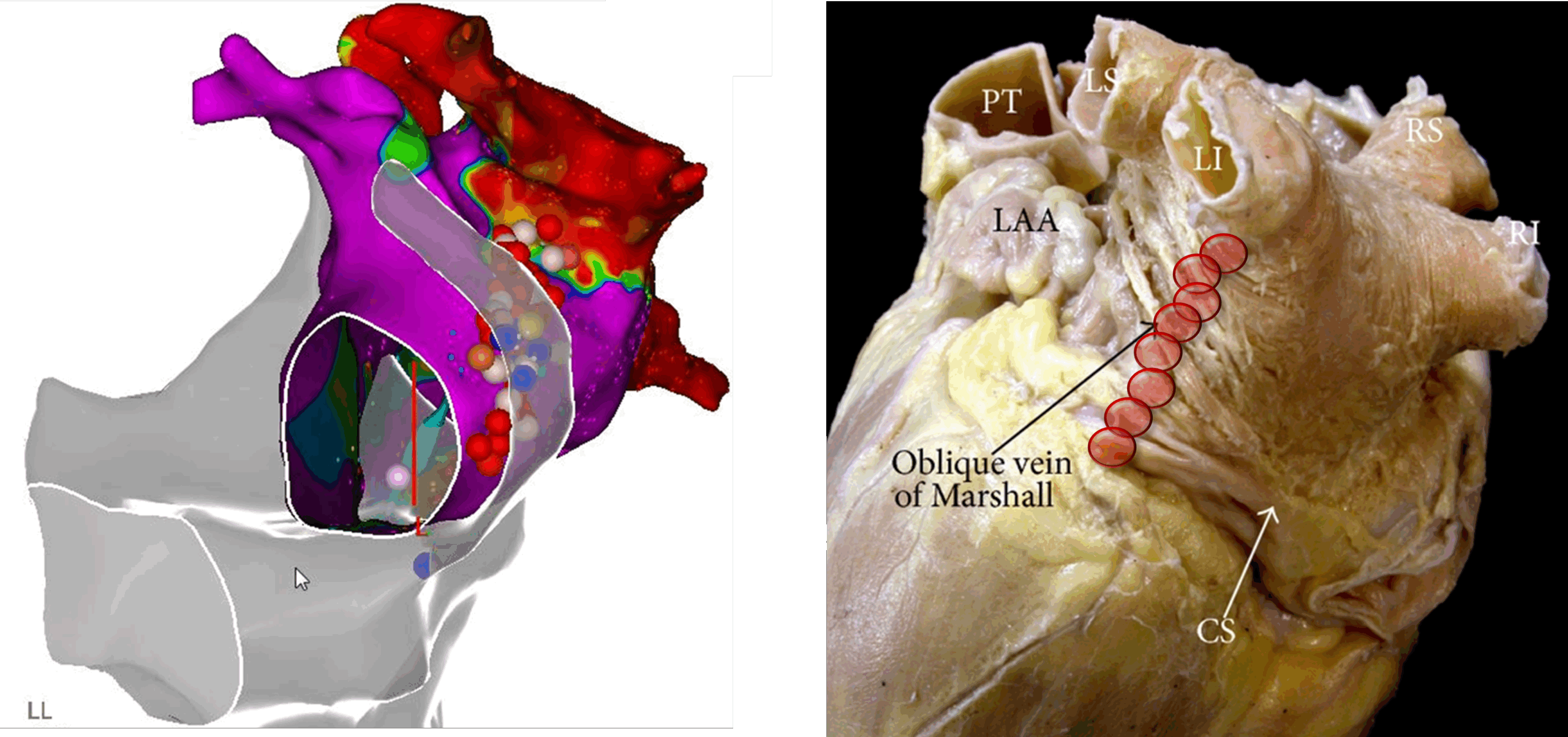
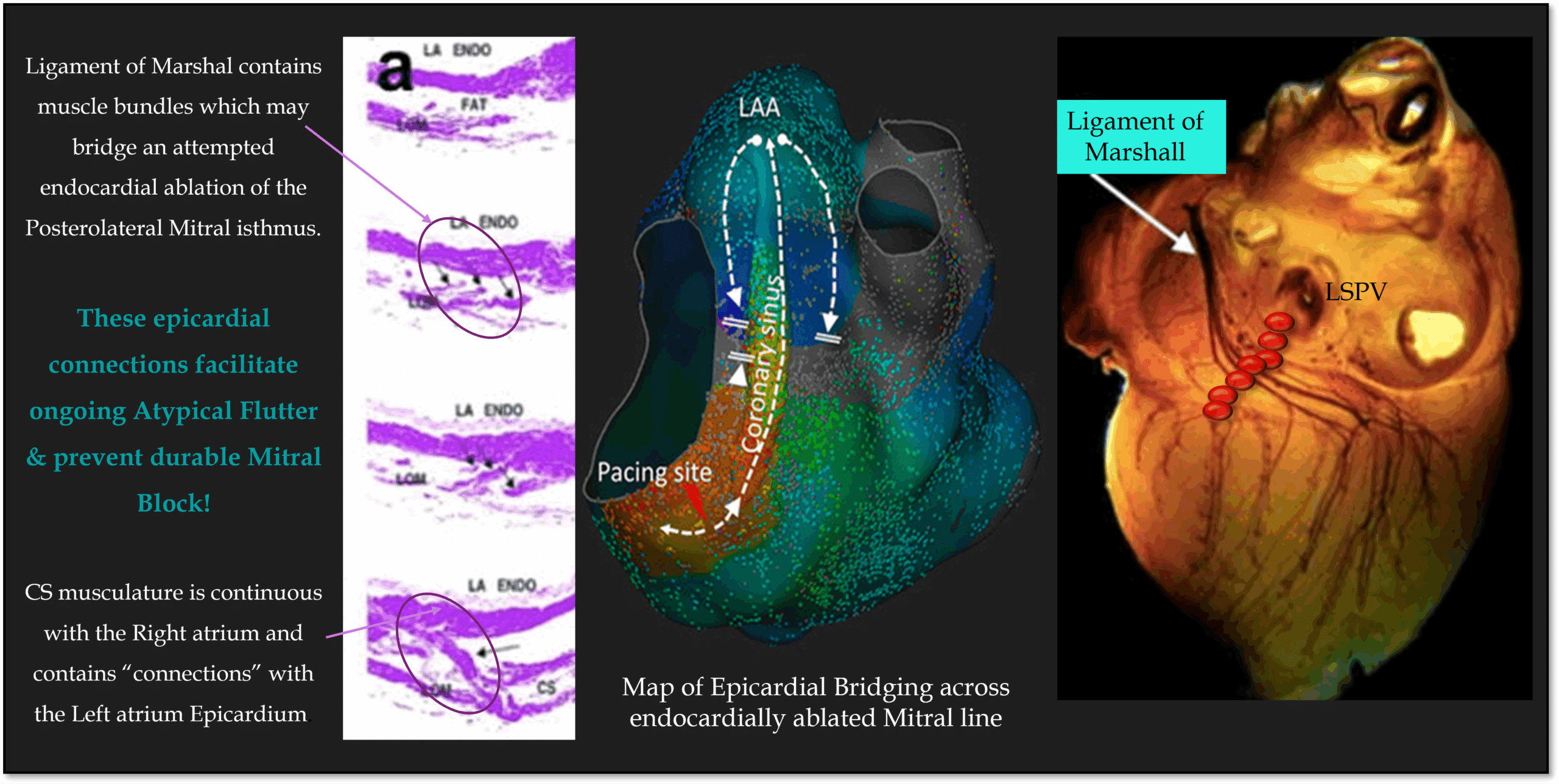
The below image also demonstrates that the Coronary Sinus and the Ligament of Marshall are two epicardial structures which epicardially bridge the Posterolateral Mitral Isthmus.
Figure adapted from: Sánchez-Quintana D, et al. 2014
These structures can contain epicardial musculature which can carry conduction across the posterolateral mitral isthmus line, even when an endocardial left atrial ablation has been performed.
Consequences of Failure to achieve Block across the Mitral isthmus
Because of these Epicardial structures, endocardial ablation alone often fails to achieve acute block in 60-70% of cases!
Patients with a failed MI line are about twice as likely to have inducible MI‑dependent flutter & >triple the risk of clinical arrhythmia recurrence versus patients with durable block (57.1% vs 18.4%)
In my view, this translates to: “Do not attempt this line unless you are prepared to burn epicardially, or use adjunctive ablation methodologies such as Ligament of Marshall alcohol ablation”
Figure adapted from: Rodríguez-Mañero M, et al. 2016; Valderrábano M. 2018; Sánchez-Quintana D, et al. 2014
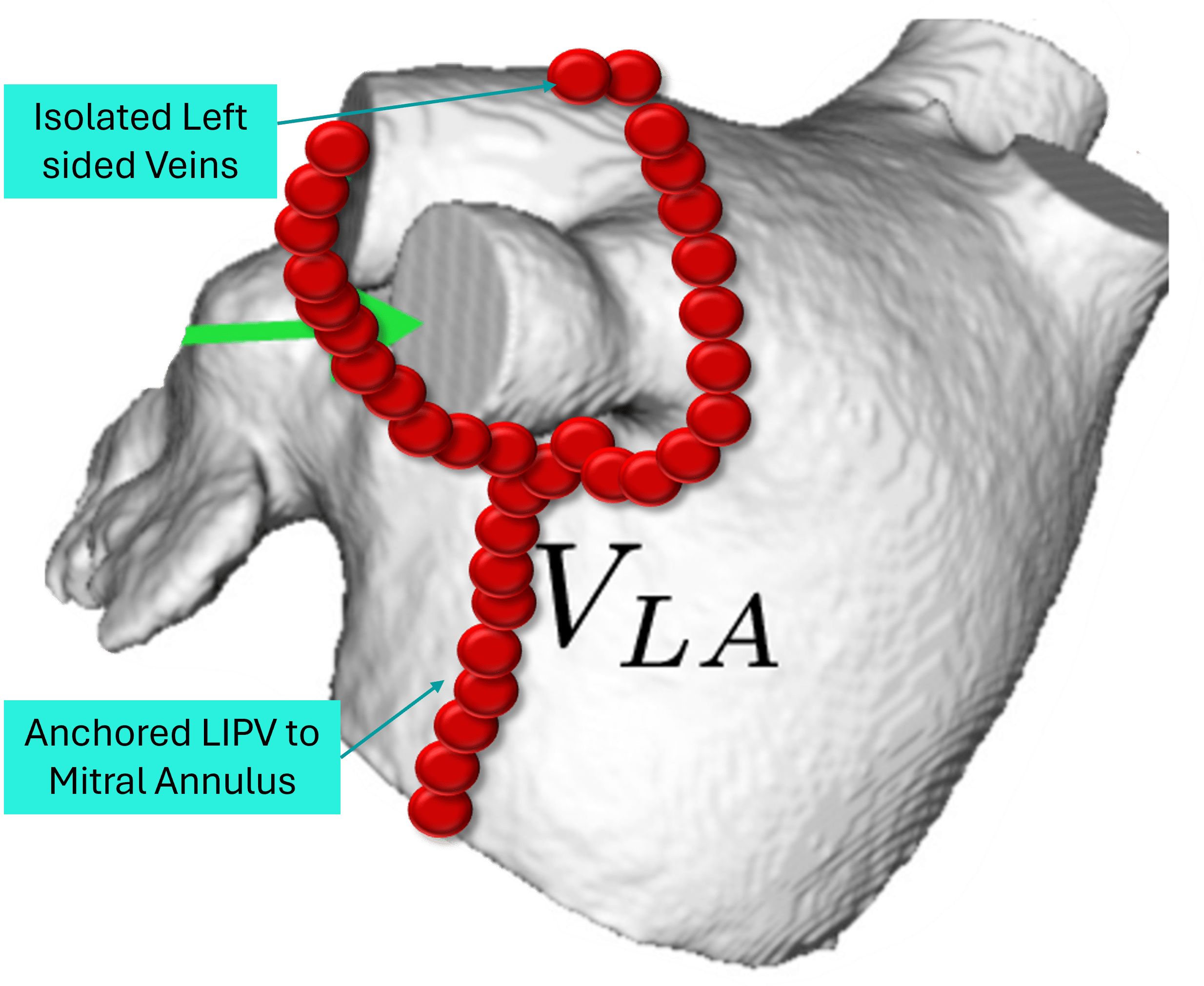
How to achieve durable block across the Posterolateral Mitral Isthmus
Step 1: Endocardial Ablation
Anchor an isolated LIPV to the Mitral Annulus endocardially.
Step 2: Coronary Sinus Epicardial Ablation
Performing an epicardial Ablation line, directly opposite the endocardial ablation line, increases the chance of successfully blocking the Posterolateral Mitral Isthmus, however this is at the risk of:
Injuring the Left Circumflex Artery
Causing life threatening CS perforation & possible tamponade.
Ablation settings should take into consideration the thin CS sleeves & risk of perforation & ideally be <25watts with relatively short duration & care taken to avoid excessive contact force.
Figure adapted from: Wong KC, et al. 2011 Aug;32(15):1881-90.
Step 3: If still not blocked – map the earliest EGM breakthrough
Ideally this can be done during Clockwise Mitral Flutter or LAA Pacing.
Map the earliest EGM on the LA Endocardium – to map endocardial or epicardial LA breakthrough. (Figure 1)
Map the earliest EGM within the CS – mapping possible epicardial breakthrough across the MI line (Figure 2).
Figure adapted from: Mechulan A, et al. 2024 Apr 11
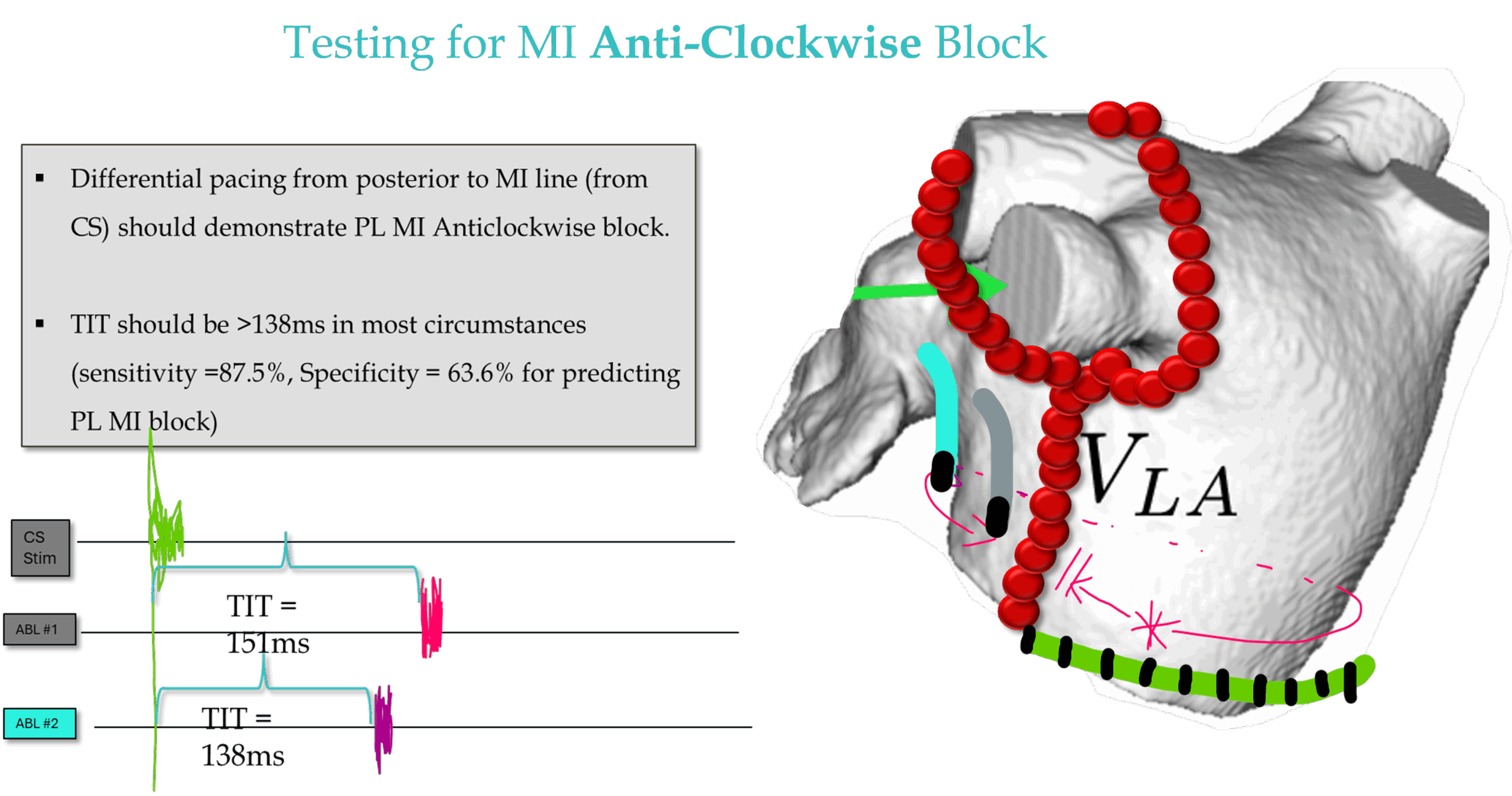
Testing for MI Block:
Anticlockwise block can be tested by pacing from the CS & performing differential mapping anterior to the posterolateral MI line.
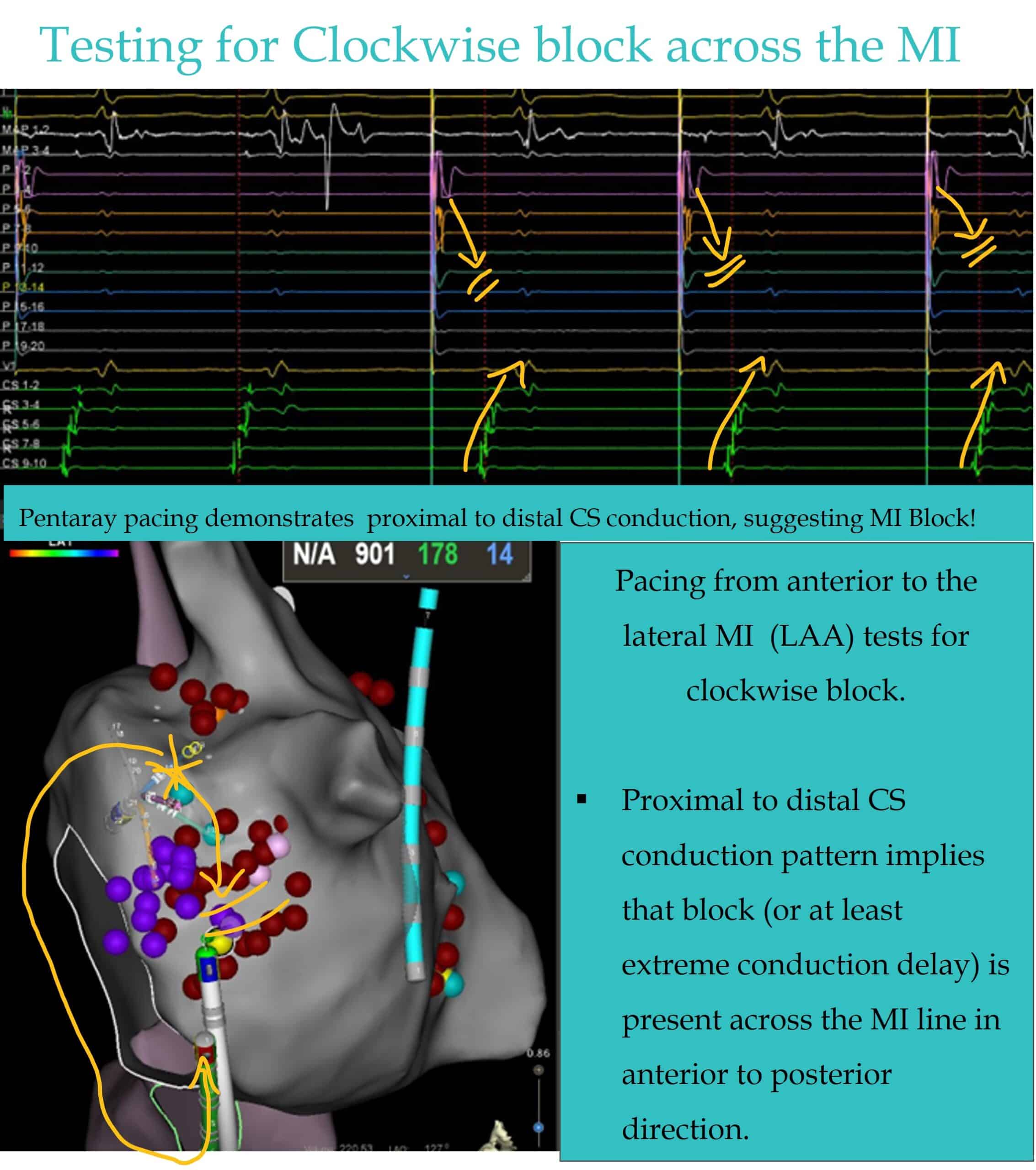
Clockwise Block can be demonstrated with LAA pacing & noting the CS conduction pattern.
Overview of Steps
My Two Cents:
Up to 70% of Posterolateral MI lines fail to achieve block with empiric endocardial LA ablation alone.
Failed MI lines cause harm & are proarrhythmic.
Epicardial Ablation within the CS, & mapping epicardial breakthrough during pacing is often necessary to achieve durable MI block.
Epicardial ablation risks CS perforation & LCx injury – all of which may be life threatening.
Ligament/Vein of Marshall Ethanol infusion has demonstrated efficacy as an adjunct to ablation in achieving durable MI block, however, carries it’s own risks of tamponade & complications.
Don’t begin an endocardial Posterolateral MI line ablation unless you are prepared to fail and progress to a more aggressive, higher risk strategies to achieve durable block.
Thanks for tuning in :)
Cheers
Mitch & CPiP team
This post was based on lectures found in Program 3 & Program 5 of EP in Practice. No Compromises. No Shortcuts. Just EP Mastery.
Sánchez-Quintana D, López-Mínguez JR, Macías Y, Cabrera JA, Saremi F. Left atrial anatomy relevant to catheter ablation. Cardiol Res Pract. 2014;2014:289720.
Barkagan M, Shapira-Daniels A, Leshem E, Shen C, Anter E. Pseudoblock of the Posterior Mitral Line With Epicardial Bridging Connections Is a Frequent Cause of Complex Perimitral Tachycardias. Circ Arrhythm Electrophysiol. 2019 Jan;12(1):e006933.
Cabrera JA, Ho SY, Climent V, Sanchez-Quintana . The architecture of the left lateral atrial wall: a particular anatomic region with implications for ablation of atrial fibrillation. Eur Heart J. 2008; 29:356–362.
Wong KC, Lim C, Sadarmin PP, Jones M, Qureshi N, De Bono J, Rajappan K, Bashir Y, Betts TR. High incidence of acute sub-clinical circumflex artery ‘injury’ following mitral isthmus ablation. Eur Heart J. 2011 Aug;32(15):1881-90.
Hamoud NS, Abrich VA, Shen WK, Mulpuru SK, Srivathsan K. Achieving durable mitral isthmus block: Challenges, pitfalls, and methods of assessment. J Cardiovasc Electrophysiol. 2019 Sep;30(9):1679-1687.
Mechulan A, Dieuzaide P, Peret A, Vaugrenard T, Houamria S, Pons F, Nait-Saidi L, Miliani I, Lemann T, Bouharaoua A, Prévot S. Strategy to achieve mitral isthmus flutter ablation by radiofrequency: the SHERIFF plan. J Interv Card Electrophysiol. 2024 Apr 11.
Rodríguez-Mañero M, Schurmann P, Valderrábano M. Ligament and vein of Marshall: A therapeutic opportunity in atrial fibrillation. Heart Rhythm. 2016 Feb;13(2):593-601 Valderrábano M. Ligament of Marshall arrhythmogenesis and vein of Marshall ethanol: A problem with a solution. Heart Rhythm. 2018 Jan;15(1):25-27
Valderrábano M. Ligament of Marshall arrhythmogenesis and vein of Marshall ethanol: A problem with a solution. Heart Rhythm. 2018 Jan;15(1):25-27.
Li X, Liu T, Cui B, Zhang J, Chen Y, Wu G. Efficacy and Safety Ablation Index-Guided High-Energy Linear Ablation for Persistent Atrial Fibrillation: PVI Plus Linear Ablation of Mitral Isthmus and Posterior Box Isolation. J Clin Med. 2023 Jan 12;12(2):619.
Lim TW, Koay CH, See VA, McCall R, Chik W, Zecchin R, Byth K, Seow SC, Thomas L, Ross DL, Thomas SP. Single-ring posterior left atrial (box) isolation results in a different mode of recurrence compared with wide antral pulmonary vein isolation on long-term follow-up: long survival time but similar survival time free of any atrial arrhythmia. Circ Arrhythm Electrophysiol. 2012 Oct;5(5):968-77.ger atrial fibrillation-free
Cho Y, Lee W, Park EA, Oh IY, Choi EK, Seo JW, Oh S. The anatomical characteristics of three different endocardial lines in the left atrium: evaluation by computed tomography prior to mitral isthmus block attempt. Europace. 2012 Aug;14(8):1104-11.