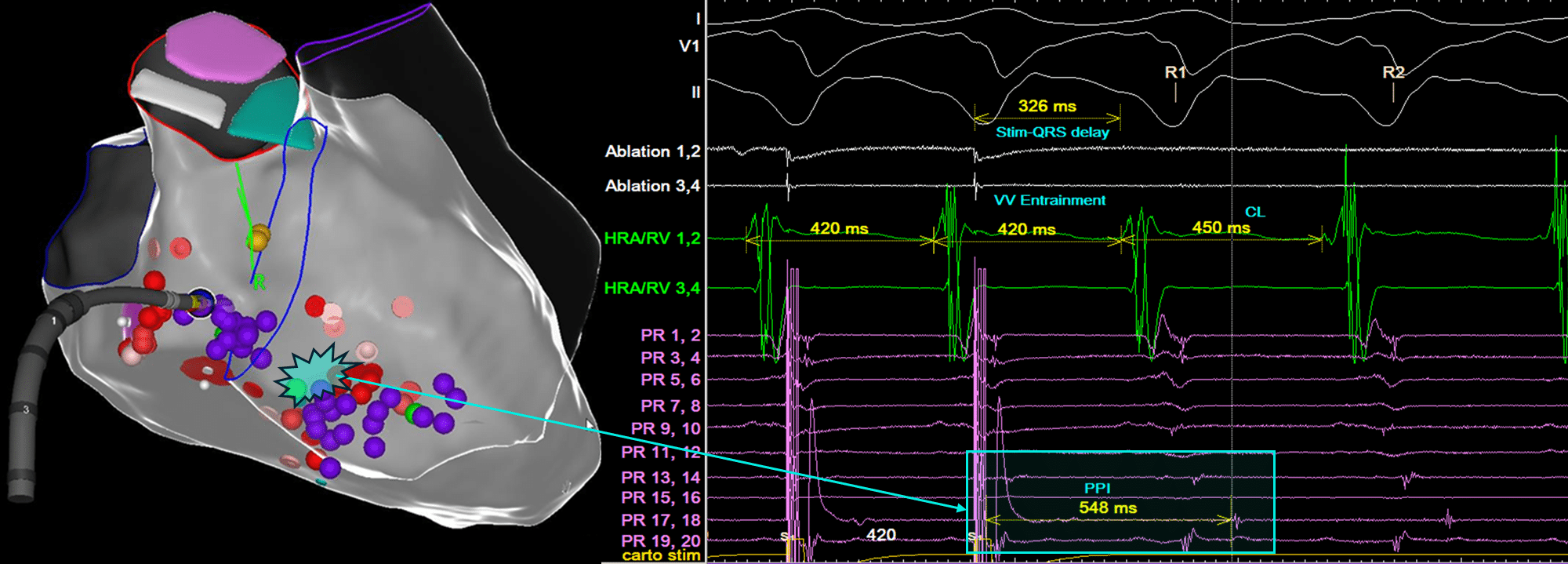
This EGM was obtained during an attempt at VT entrainment of haemodynamically stable monomorphic VT. The pacing site was thought to be within a region of scar that may be involved in the VT circuit. Given this EGM, would ablation in this location likely terminate the VT?
(Click to zoom on image)
Answer:
Click to Show Answer
Answer: Successful VT entrainment within a constrained adjacent bystander site. Unlikely to terminate tachycardia becase pacing site is remote from the tachycardia circuit due to the long Post Pacing Interval.
VT Entrainment pros and cons
Entrainment in Scar VT is a complex topic and unfortunately, not routinely practiced in the EP lab for a number of reasons. The first and most dominant reason, is that VT is usually haemodynamically unstable, so entrainment mapping is not possible. The second reason is that we have many other tools at our disposal that help us direct our ablation strategy.
Despite this, VT entrainment remains the ONLY definitive method of confirming VT isthmus site location.
VT Entrainment simplified:
To simplify things, we shall assume a reentrant mechanism of VT. In this case, there are 3 things to look out for and measure during VT entrainment.
Is there concealed or manifest fusion?
Is there a Stim-QRS delay?
What is the PPI -TCL?
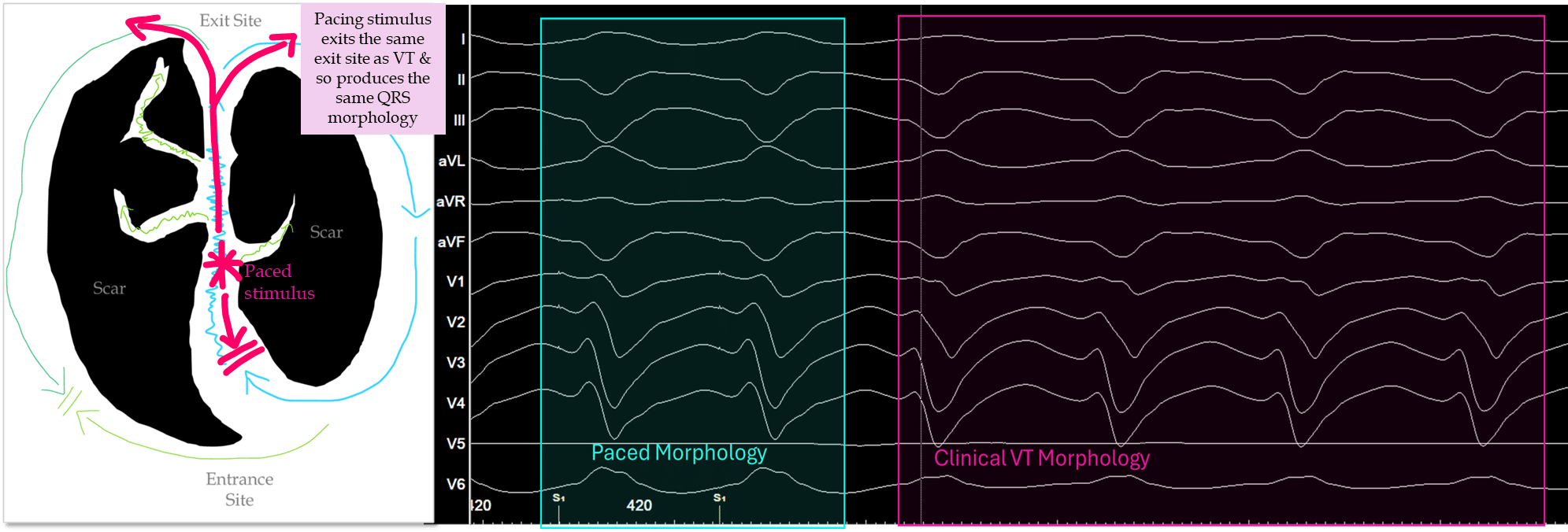
Firstly: Is there concealed or Manifest Fusion?
Concealed fusion is when entrainment successfully acclerates the tachycardia CL to the pacing CL, but does not appreciably alter the VT morphology during pacing.
The pacing stimulus should EXACTLY match the VT morphology.
If it doesn’t match EXACTLY, then this is called “Manifest fusion” and indicates your pacing stimulus is not using the same exit site as the VT reentrant circuit and therefore ablation at your pacing site is unlikely to terminate tachycardia.
Example of Concealed fusion below:
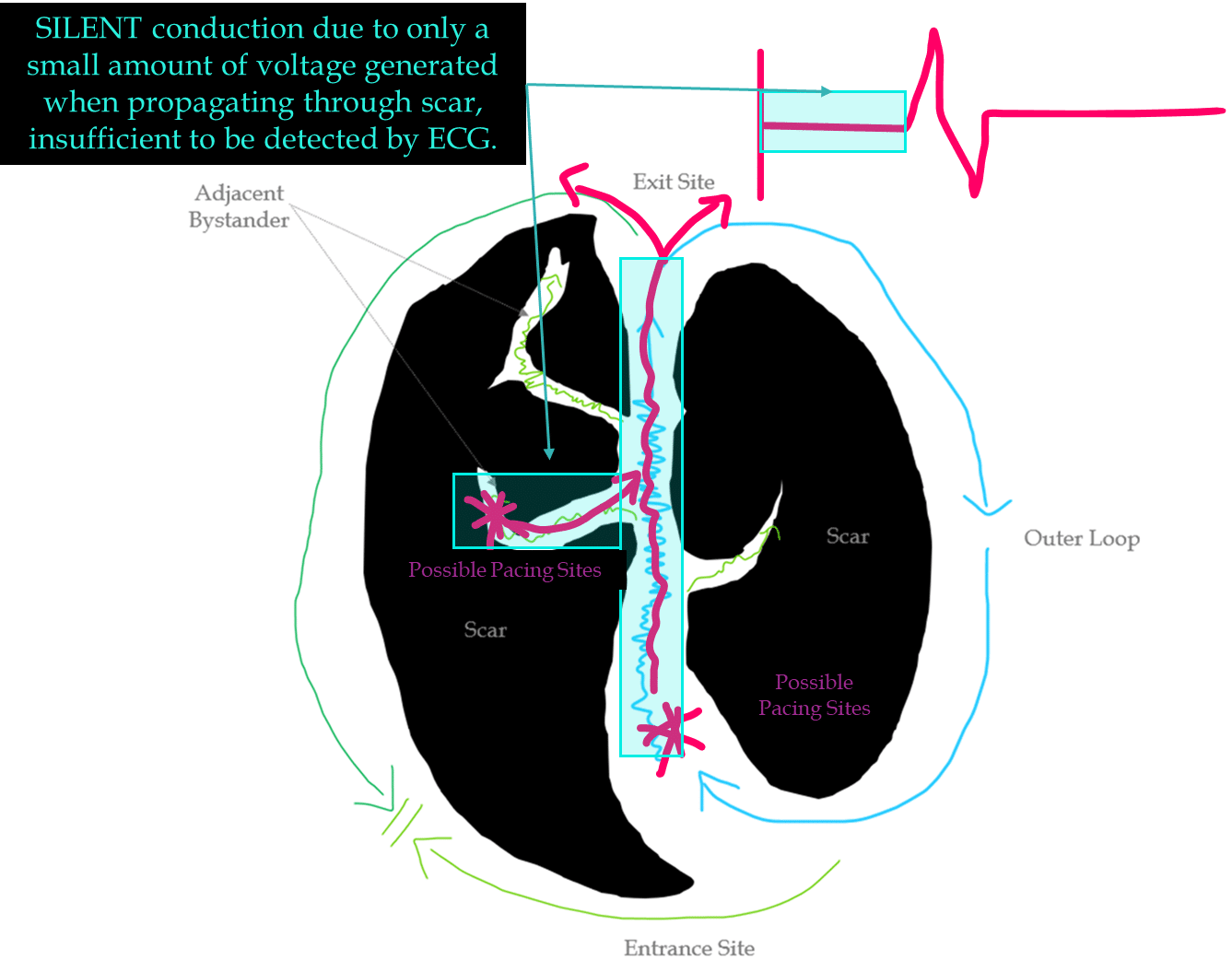
Secondly: Is there a Stim -QRS delay?
Stim-QRS delay <30% of TCL = EXIT Site or Adjacent Bystander
Stim – QRS delay 30-50% of TCL = Isthmus site or Adjacent Bystander
Stim-QRS delay >50% of TCL = Entrance site or Adjacent Bystander
In our example above, the stim-QRS delay is 326ms (73%). Indicating an entrance or adjacent bystander site.
Below is a diagram showcasing some possible pacing sites based on concealed fusion with a long stim to QRS.
Notice, that ablation at the lower pacing site will likely terminate VT.
But ablation at the adjacent bystander site would not provide benfit.
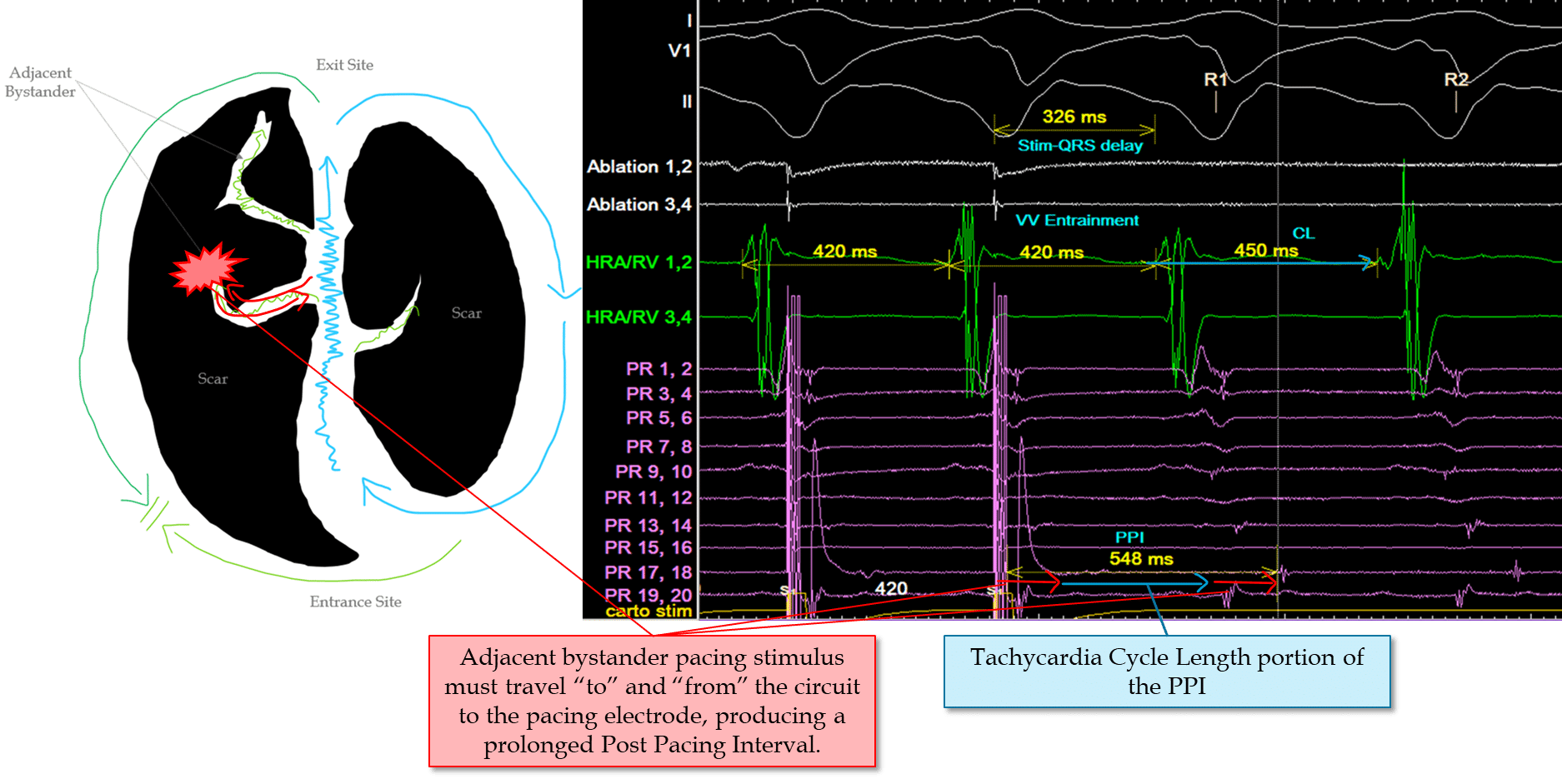
Thirdly: PPI – TCL – the ONLY way of proving our pacing site is involved in the circuit.
The PPI is measured from the pacing electrode, to the return EGM on the same electrode.
Care must be taken if there are multiple discrete EGM’s, (such as double potentials) on the same electrode. Efforts should be made to ensure you measure to the same EGM you captured with the pacing stimulus.
PPI – TCL <30ms indicates your pacing site within the circuit.
This could be an entrance site, an outer loop, an exit site, or a critical isthmus site.
Only SOME of these locations will terminate VT if ablation is attempted.
This is why we must also consider “concealed fusion” and stim-QRS delay alongside the PPI – TCL measurement.
Summing up the evidence in our EGM of Question:
Evidence of concealed fusion
Indicates pacing within constrained scar using the same exit site as VT.
Pacing site NOT part of the circuit (so not entrance site).
Adjacent bystander site!!!!!!!!!
My Two Cents:
VT entrainment measurements hinge on x3 things.
Concealed fusion
Stim-QRS delay
PPI – TCL
In my opinion, analaysing VT entrainment in that order (assuming you have successfully accelerated the VT) helps you methodically deduce where you’re pacing site is relative to the tachycardia circuit.
VT entrainment is a complex phenomenon, but it’s measurement in the EP lab can be simplified into those steps for rapid “on the fly” analysis.
Stevenson WG, Khan H, Sager P, Saxon LA, Middlekauff HR, Natterson PD, Wiener I. Identification of reentry circuit sites during catheter mapping and radiofrequency ablation of ventricular tachycardia late after myocardial infarction. Circulation. 1993 Oct;88(4 Pt 1):1647-70.
Stevenson WG, Friedman PL, Sager PT, Saxon LA, Kocovic D, Harada T, Wiener I, Khan H. Exploring postinfarction reentrant ventricular tachycardia with entrainment mapping. J Am Coll Cardiol. 1997 May;29(6):1180-9. doi: 10.1016/s0735-1097(97)00065-x. PMID: 9137211.
Gustavo S. Guandalini, Jackson J. Liang, Francis E. Marchlinski, Ventricular Tachycardia Ablation: Past, Present, and Future Perspectives, JACC: Clinical Electrophysiology, Volume 5, Issue 12, 2019,Pages 1363-1383
Tung R. Challenges and Pitfalls of Entrainment Mapping of Ventricular Tachycardia: Ten Illustrative Concepts. Circ Arrhythm Electrophysiol. 2017;10(4):e004560.