Sometimes, ablation at excellent pacemap sites fail to abolish reentry VT. Good pacemaps can misleadingly arise in bystander sites and other sites that are NOT involved in VT reentry.
So how can pacemapping reliably identify a critical diastolic isthmus site - and differentiate an endocardial isthmus site vs intramural reentry circuit?
(Click to zoom on image)
Answer:
Click to Show Answer
The Basic concepts of pacemapping in Scar-VT:
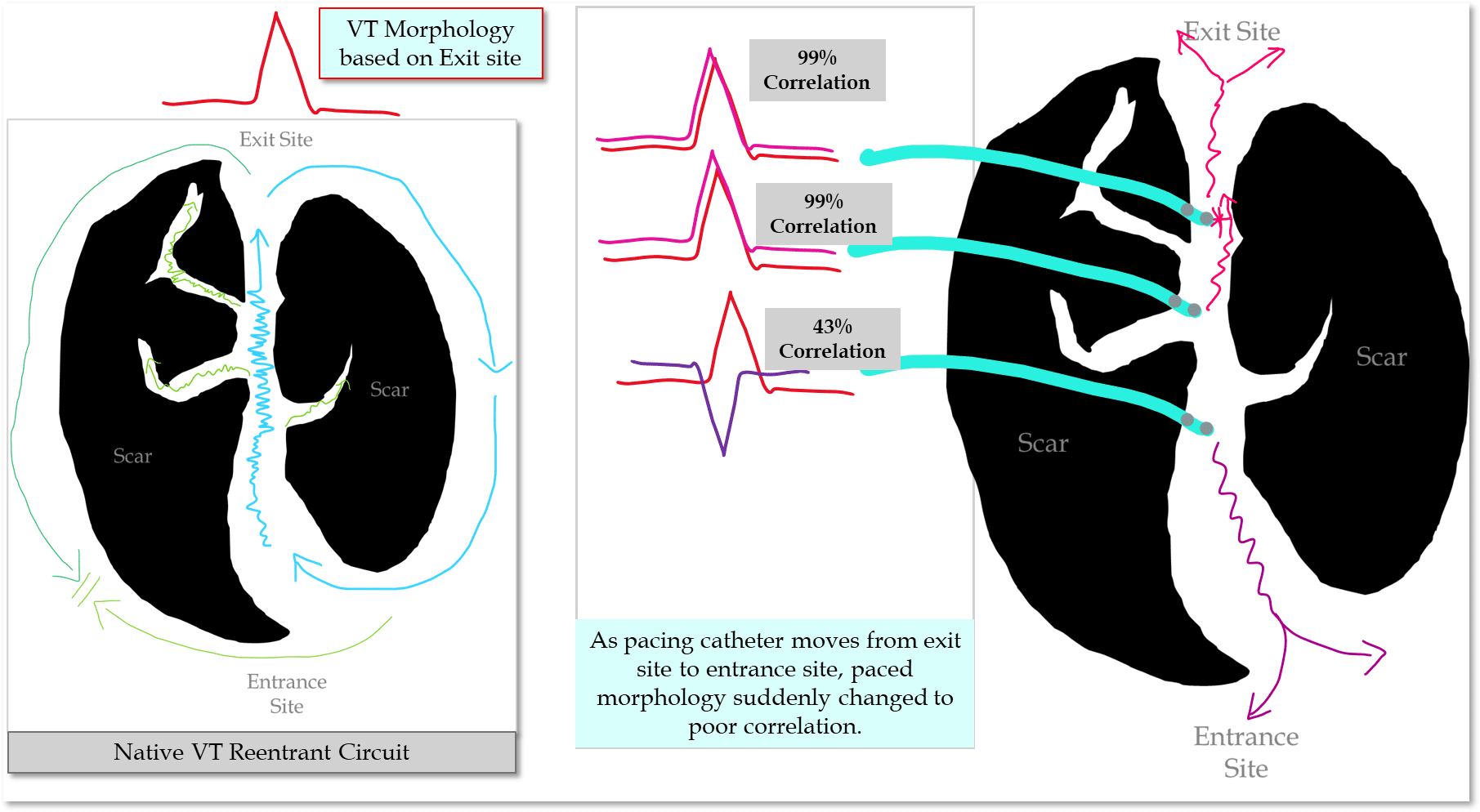
Identifying pacemap QRS morphologies with a high correlation (>95%) to the VT morphology indicates you are pacing from the exit site.
Both an adjacent bystander and critical isthmus site may display:
Long stim-QRS
High correlation to VT morphology
What will be discussed here:
Sudden changes in paced morphologies in two anatomically adjacent sites predicts an endocardial critical isthmus site.
Centrifugal patterns of pace-map correlations indicate an intramural circuit.
These factors inform ablation strategy
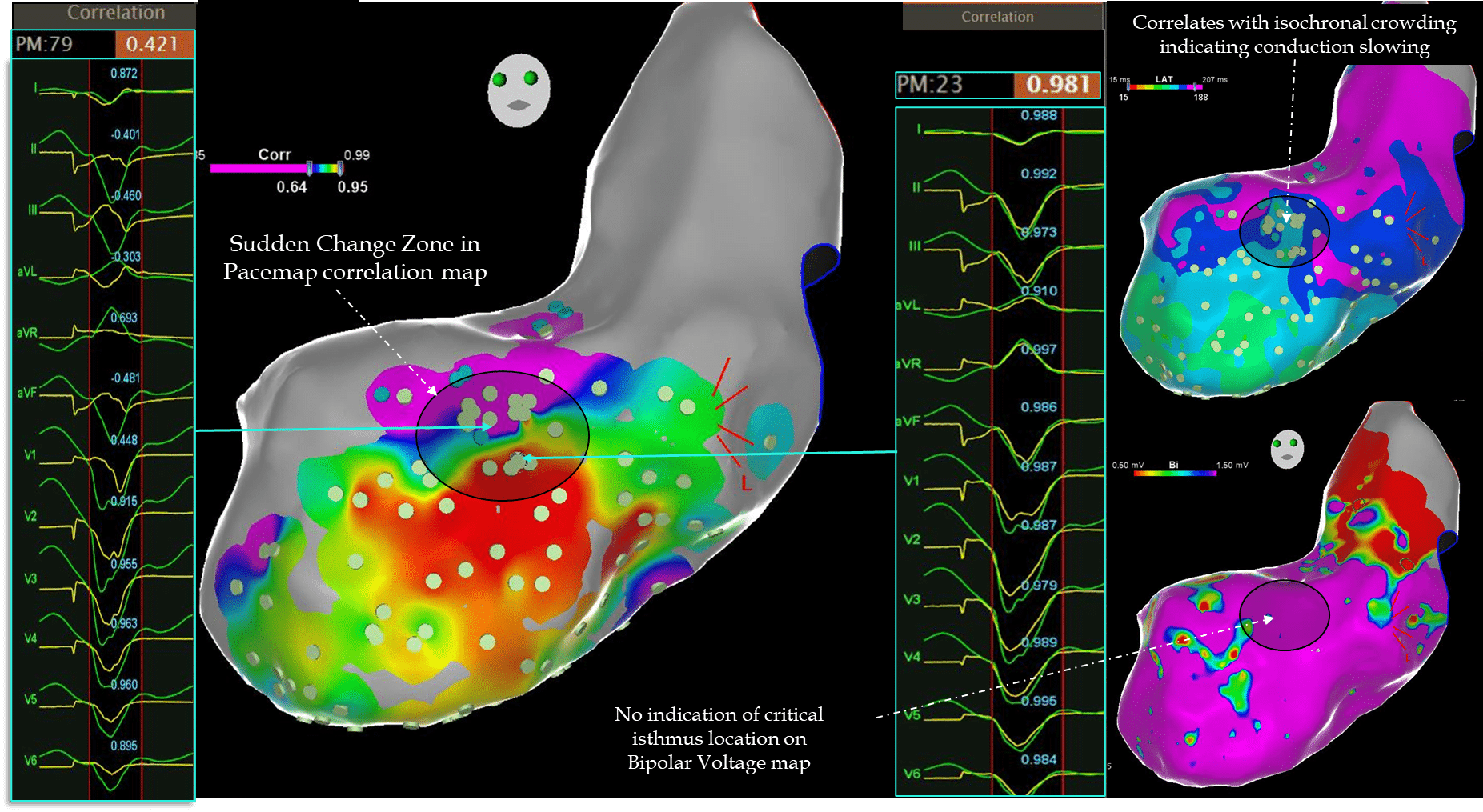
An example of a “Sudden Change” in Pacemap Morphology
Key Concept!
An abrupt 30% change in pacing correlation from a good pacemap to a poor pacemap correlates with a specifically endocardial diastolic isthmus sites critical for maintaining VT re-entry circuits.
Why does a sudden change pattern correlate with an endocardial isthmus site?
No sudden change = No Isthmus site :(
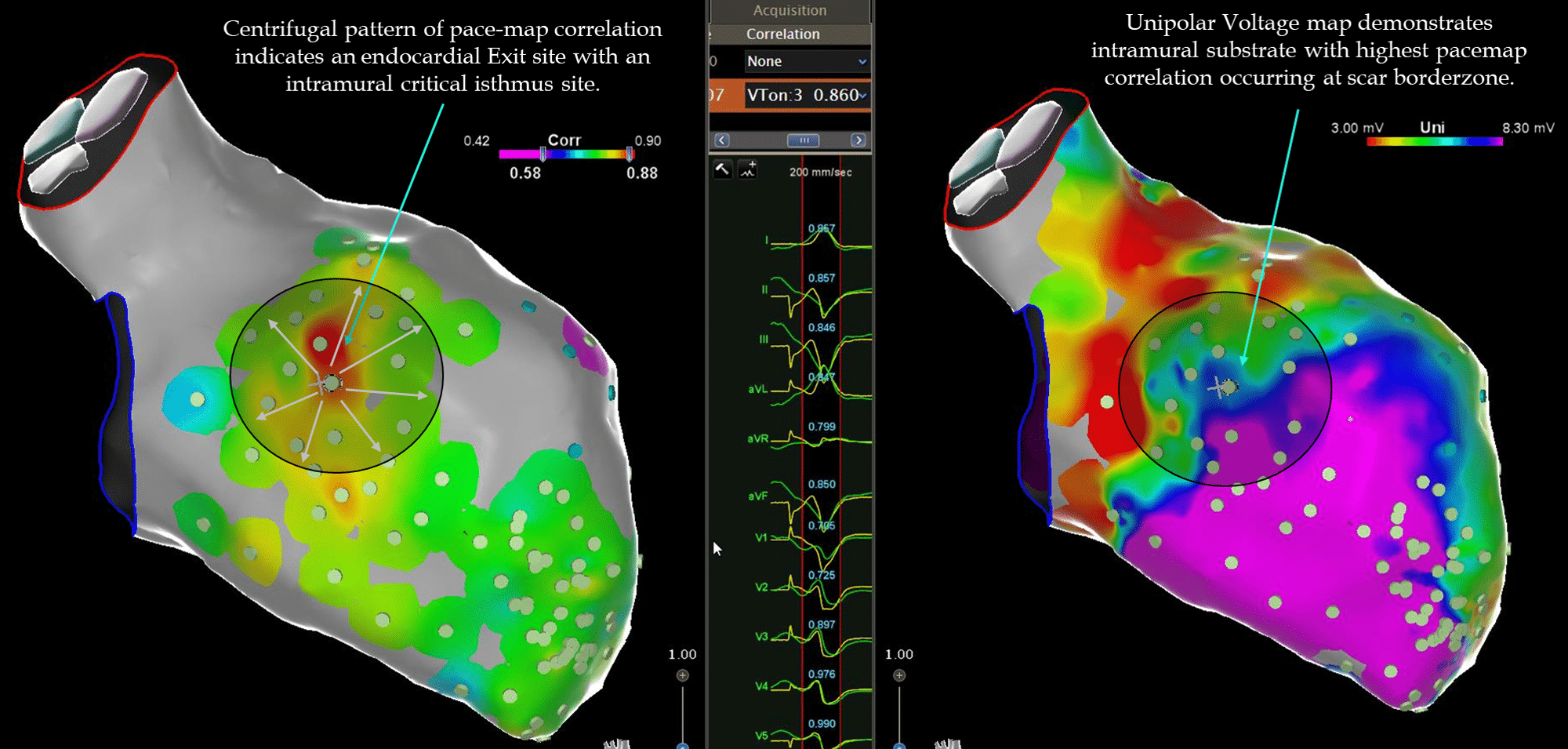
If an abrupt change pattern is not seen, then you will likely obtain a “centrifugal pattern” of pacemap correlation (example below).
The pacemap correlation gradually becomes worse as you pace further from the exit site in all directions.
A centrifugal pacemap correlation map indicates an intramural or epicardial isthmus site (when performing pacemapping from the endocardium).
An example of a centrifugal pattern of pacemap correlations is demonstrated in the example below, where the VT isthmus site was intramurally located.
My Two Cents:
VT is often a 3-dimnentional re-entrant circuit involving the intramural substrate.
In my opinion, in many centres, pacemapping is both underutilised & underappreciated in scar VT ablations.
It can reliably identify endocardial critical isthmus sites in unstable VT, or indicate the presence of an intramural circuit.
A sudden change in pacemap morphology (>30% correlation) from good to bad pace-map at two anatomically adjacent sites strongly correlates with the location of an endocardial critical diastolic isthmus site.
In contrast, a centrifugal pattern of gradually poorer pace-map morphology indicates an intramural critical isthmus site and possibly a more difficult endocardial ablation.
Thanks for tuning in :)
Cheers
Mitch & CPiP Team
Start your structured journey to mastering EP in 2 years with EP in Practice.
(SEMINAL PAPER RECOMMENDED) De Chillou C, Groben L, Magnin-Poull I et al. Localizing the critical isthmus of postinfarct ventricular tachycardia: the value of pace-mapping during sinus rhythm. Heart Rhythm. 2014;11:175–81
Sadek MM, Schaller RD, Supple GE, Frankel DS, Riley MP, Hutchinson MD, Garcia FC, Lin D, Dixit S, Zado ES, Callans DJ, Marchlinski FE. Ventricular Tachycardia Ablation – The Right Approach for the Right Patient. Arrhythm Electrophysiol Rev. 2014 Nov;3(3):161-7.
Sadek MM, Schaller RD, Supple GE, Frankel DS, Riley MP, Hutchinson MD, Garcia FC, Lin D, Dixit S, Zado ES, Callans DJ, Marchlinski FE. Ventricular Tachycardia Ablation – The Right Approach for the Right Patient. Arrhythm Electrophysiol Rev. 2014 Nov;3(3):161-7.
2 Responses
Loving the content Mitch👍🏼
Thanks Anugrah that means a lot! Glad you’re enjoying it 🙂