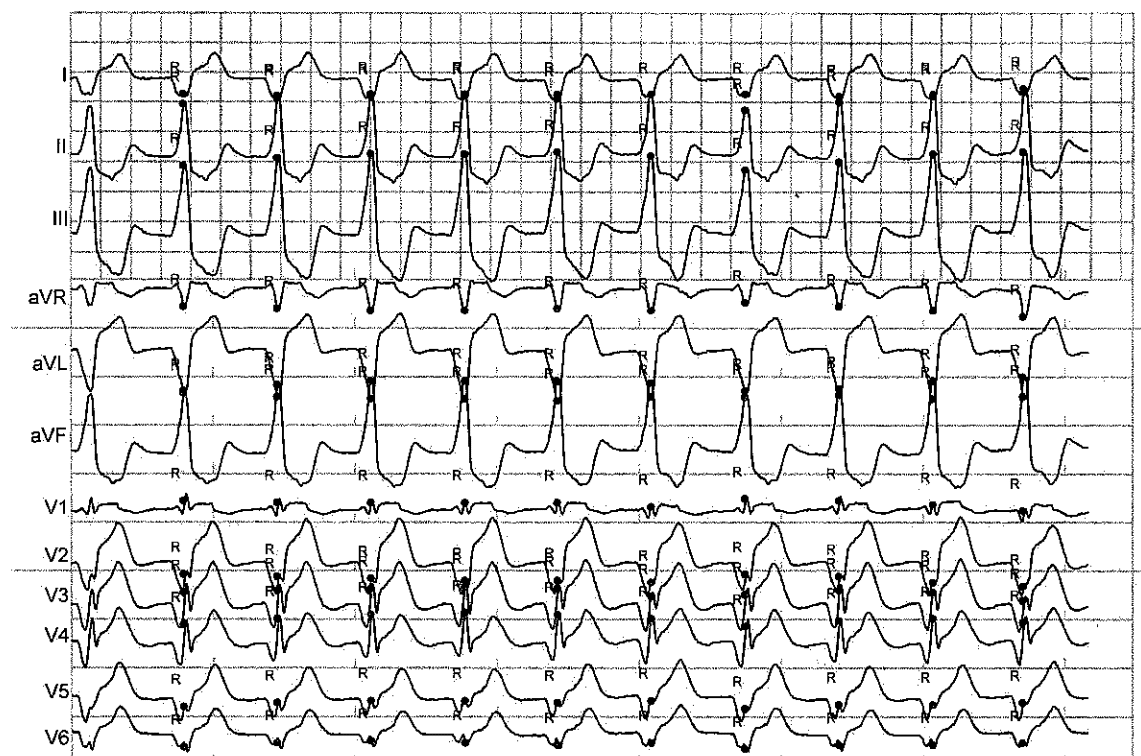
58 year old male presented with an occlusive anterior infarct with symptoms of hypotension, diaphoresis, & central chest tightness. During emergency PCI, blood flow was restored after angioplasty. 4 minutes after LAD reperfusion, the rhythm below initiated.
What is the mechanism & prognosis of the rhythm below?
(Click to zoom on image)
Answer:
Click to Show Answer
Answer: Accelerated Idioventricular Rhythm (AIVR) secondary to Reperfusion injury.
Accelerated Idioventricular Rhythm (AIVR)?
Accelerated idioventricular rhythm refers to ventricular ectopic rhythm between 40-100bpm. It is usually a wide QRS complex, (sometimes looking like a bundle branch block if it arises from purkinjie tissue near a bundle branch) with either AV dissociation or VA conduction (rerograde P waves).
This rhythm is exceedingly common following reperfusion of a patient with Occlusive Myocardial Infarction & often (but not always) produce a ventricular rhythm with a QRS morphology which reflects the region of infarct/ishaemia.
Symptoms of AIVR
Lack of AV synchrony results in patients experiencing “pacemaker syndrome” which is essentially a cluster of symptoms caused by AV dissociation (sometimes seen in suboptimally programmed pacemaker patients -hence the name) including hypotension, dyspnoea, coughing, feelings of choking, nausea, dizziness, neck pulsations and headache.
In the example below, you can see the inverted retrograde P waves highlighted in the inferior leads. This patient was “coughing” & agitated every time they reverted to AIVR rhythm.
Clinical Presentation of Reperfusion Arrhythmias.
Reperfusion Arrhythmia following reperfusion of the ischaemic myocardium manifests most commonly as VT, VF, AF, Sinus Tachy or AIVR, particularly if performed abruptly after 15–20 min of ischaemia.
Patients may continue to exhibit reperfusion arrhythmias for up to 48 hours after reperfusion. Although the vast majority of them are well tolerated, VT or VF can be haemodynamically unstable, especially when complicated by MI and are associated with higher mortality. Reperfusion arrhythmias are predominantly observed following a brief ischemic duration, when the myocardium has not permanently necrosed & reperfusion restores some myocardial function.
In the thrombolytic era, or when PCI is not available, these arrhythmias occurring within 6 hours of thrombolysis were defined as noninvasive indicators of early coronary reperfusion, and thought to be positive indicators of prognosis (After all – dead tissue does not produce automatic arrhythmias).
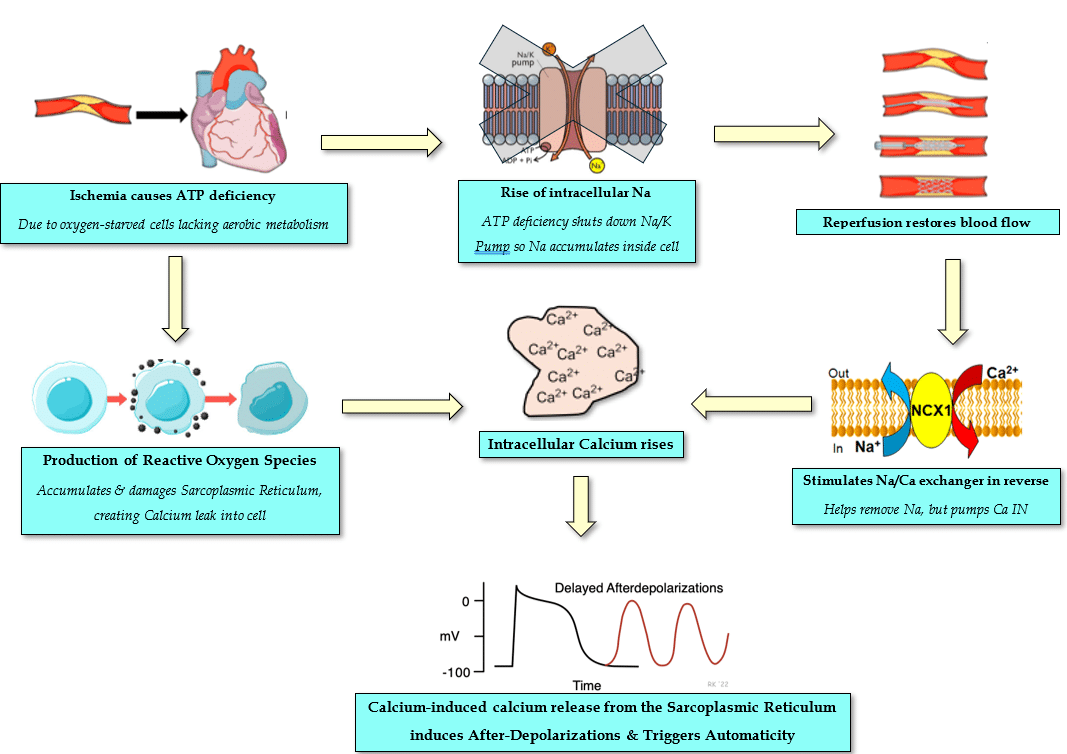
Mechanisms of Reperfusion Arrhythmias
Many reperfusion arrhythmias are mediated by calcium overload resulting in enhanced automaticity/triggered activity arrhythmias (mechanism outlined above).
Some literature suggests reperfusion injury promotes greater transmural dispersion of refractoriness leading to re-entry based ventricualr arrhythmias including ventricular fibrillation.
Prognosis of Reperfusion Arrhythmias:
One study found that 97% of patients with acute anterior MI who underwent primary PCI developed at least one ventricular reperfusion arrhythmia, with nonsustained VT, AIVR, and frequent VEB’s being the most common.
In the era of Thrombolytic treatment of Occlusive MI, reperfusion arrhythmias were thought to be positive prognostic indicators, since they implied that the myocardial tissue had not undergone a “completed infarct” but was at least partially recovering after blood flow was restored with thrombolysis. Simplistically speaking, it was thought that dead myocytes don’t generate arrhythmias, so reperfusion arrhythmias must indicate “alive” myocytes.
Some studies in the PCI era however, have found that ventricular reperfusion arrhythmias are associated with worse LV function in follow up post infarct, implying that ventricular reperfusion arrhythmias are actually a poor prognostic marker.
My Two Cents:
Reperfusion Arrhythmias commonly manifest as VT, VF or AIVR in the Cath lab in the first 48 hours after reperfusion & are driven by Calcium overloaded myocytes spontaneously depolarising.
They are usually non sustained and self-limiting, haemodynamically tolerated, and not cause for immediate concern unless there is evidence of haemodynamic compromise.
Sometimes, AIVR can be symptomatic & present similarly to “Pacemaker Syndrome”.
Reperfusion Arrhythmia was seen as an early non-invasive indicator of thrombolytic success and a positive indicator of viable myocardium in the thrombolytic era.
In the PCI era, the prognostic implications of reperfusion arrhythmias is less clear. Ventricular arrhythmias may be associated with larger infarct size and poorer LV function in follow up periods.
Yamazaki S, Fujibayashi Y, Rajagopalan RE, Meerbaum S, Corday E: Effects of staged versus sudden reperfusion after acute coronary occlusion in the dog. J Am Coll Cardiol 1986; 7: 564–72
Chiladakis J. A., Vlachos N., Patsouras N., Mazarakis A., and Manolis A. S., Usefulness of reperfusion ventricular arrhythmias in non-invasive prediction of early reperfusion and sustained coronary artery patency in acute myocardial infarction, Journal of Thrombosis and Thrombolysis. (2001) 12, no. 3, 231–236, 2-s2.0-0035728614,
Engelen D. J., Gressin V., Krucoff M. W., Theuns D. A., Green C., Cheriex E. C., Maison-Blanche P., Dassen W. R., Wellens H. J., and Gorgels A. P., Usefulness of frequent arrhythmias after epicardial recanalization in anterior wall acute myocardial infarction as a marker of cellular injury leading to poor recovery of left ventricular function, American Journal of Cardiology. (2003) 92, no. 10, 1143–1149, 2-s2.0-10744226369,oncluded that reperfusion arrhythmias are noninvasive indicators of myocardial cell damage
Kim MJ, Hur J, Ham IH, Yang HJ, Kim Y, Park S, Cho YW. Expression and activity of the na-k ATPase in ischemic injury of primary cultured astrocytes. Korean J Physiol Pharmacol. 2013 Aug;17(4):275-81.
William Fuller, Vina Parmar, Philip Eaton, James R Bell, Michael J Shattock, Cardiac ischemia causes inhibition of the Na/K ATPase by a labile cytosolic compound whose production is linked to oxidant stress, Cardiovascular Research, Volume 57, Issue 4, March 2003, Pages 1044–1051,
Thank you for this great information about reperfusion arrhythmias, something we see in the Cath Lab so very often. Will share to my fellow cath lab nurses. Thanks!
Thankyou Diah! I’m really glad you found this interesting. It’s true, we encounter it so often, we should certainly become more familiar with it’s underlying cause & consequences.
Cheers
Mitch

2 Responses
Thank you for this great information about reperfusion arrhythmias, something we see in the Cath Lab so very often. Will share to my fellow cath lab nurses. Thanks!
Thankyou Diah! I’m really glad you found this interesting. It’s true, we encounter it so often, we should certainly become more familiar with it’s underlying cause & consequences.
Cheers
Mitch