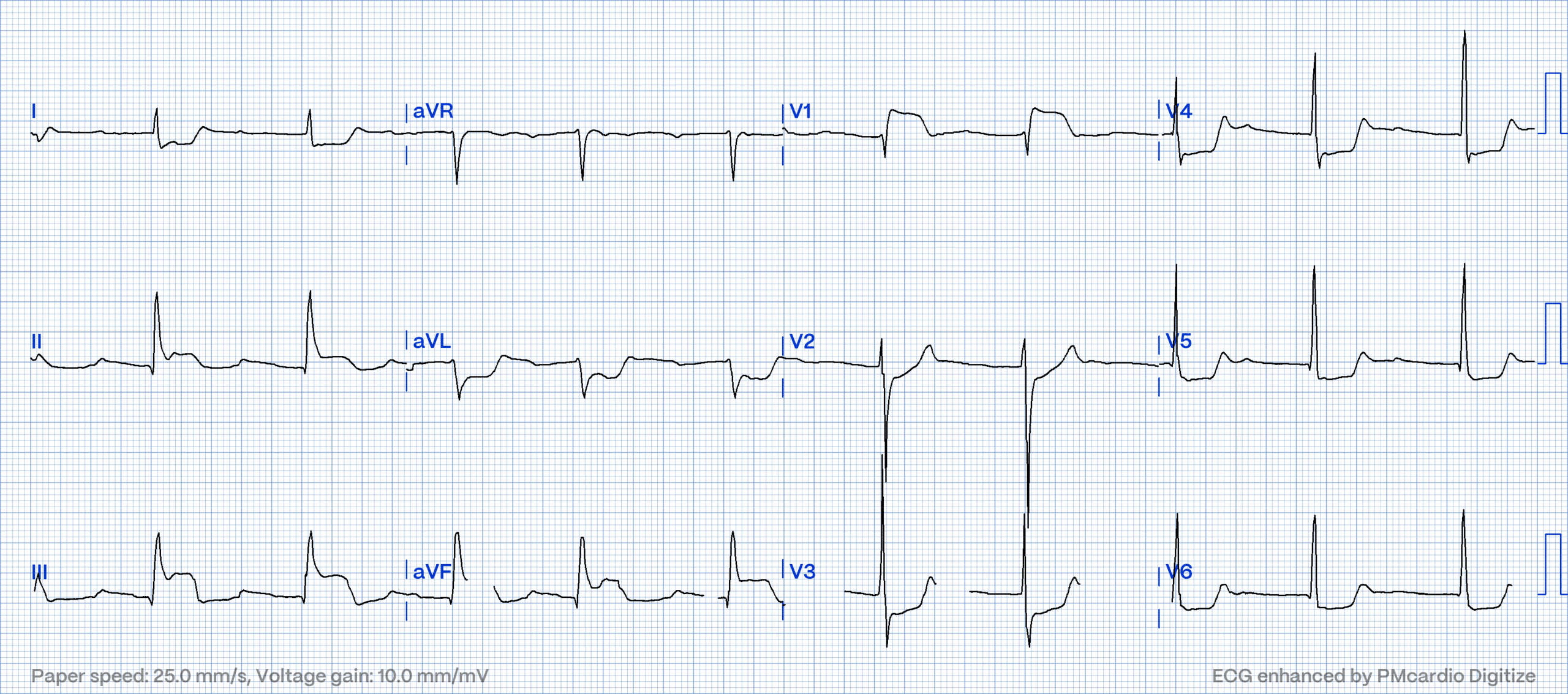
88 year old female called an Ambulance for central chest heaviness, nausea, diaphoresis & light headedness. The ECG sent by attending paramedics is shown below. What are we concerned about on this ECG?
Furthermore, are we concerned for the health of her cardiac conduction system?
(Click to zoom on image)
Answer:
Click to Show Answer
Answer – Acute inferior myocardial infarction with 3rd degree AV block, junctional escape rhythm & likely concurrent RV infarction.
ECG features indicative of diagnosis:
Occlusive inferior Myocardial Infarction:
ST elevation in II/III/aVF indicates inferior LV wall transmural ischemia.
Anterolateral reciprocal ST depression in V2-V6 is consistent with this diagnosis, further suggesting this is a true occlusive MI involving the LV inferior wall.
RV ischemia:
Furthermore, the marked ST elevation in V1 indicates a proximal RCA lesion with likely RV ischemia (see THIS Beat Box Post for more on this).
3rd degree AV Block
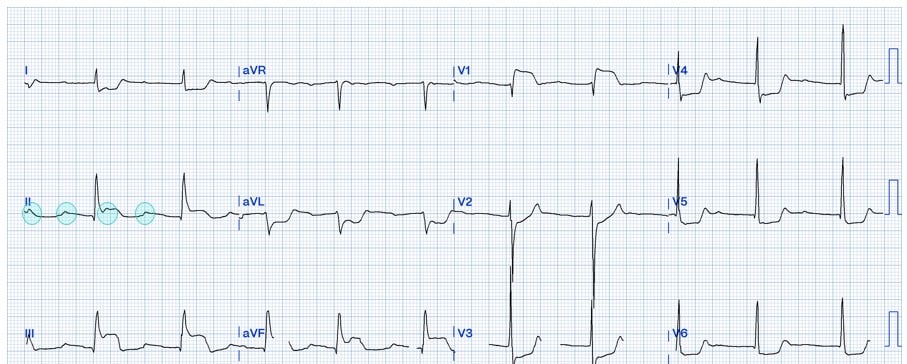
P waves can be best seen in the inferior leads, & have no relationship with the QRS complex (no consistent pattern to the “PR interval” ). This represents complete 3rd degree AV block.
Typical Inferior MI patient presentation:
Commonly: diaphoresis, feeling unwell, nauseous, hypotensive, bradyarrhythmias & general vasovagal like symptoms.
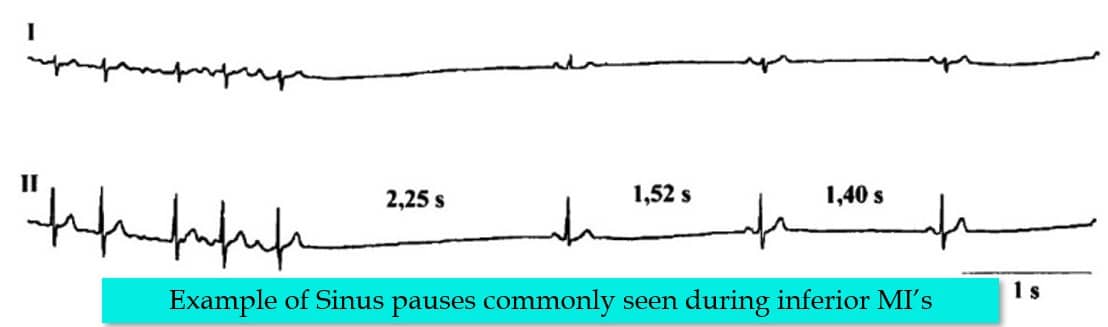
The vagal phenomena common to patients with acute inferior MI predisposes such patients to related bradyarrhythmias including:
Sinus bradycardia & pauses
Junctional rhythms (including iso-rhythmic AV dissociation)
1st AV Conduction Delay
2nd degree AV block Mobitz I & Mobitz II
CHB
Significance & Management of Bradyarrhythmias associated with an inferior MI:
Acute management:
During inferior MI, SA dysfunction or 2nd/3rd degree AV Block, are almost never permanent and almost always transient.
This is in contrast to anterior wall MI, where LAD occlusion can damage the cardiac conduction system & cause permanent bradyarrhythmias.
In the setting of inferior MI however, temporary pacing can be considered if symptomatic hypotension, dizziness, or presyncope continues despite vagolytic therapy. Temporary pacing is also sometimes used when there is concern for PVC-mediated PMVT due to persistent bradycardia & closely coupled PVC’s.
Permanent Pacing is usually indicated only if symptomatic bradyarrhythmias persist for longer than at least a few days & conventionally for more than two weeks after the MI.
Long-term management
Resist the “Oculo-Pacing reflex” – this is a phrase used by one of our contributors to our EP course, who used the term to describe the tendency for Physicians to see brady-arrhythmias and reflexively desire to implant a pacemaker.
These bradyarrhythmias are usually suprahisian & transitory in nature, very rarely permanent. Even high grade AV block usually recovers within 3-7 days of reperfusion (Trappe et al 2010).
As such, PPM implantation is likely to cause more harm than good if implantation is performed too early after inferior MI and not enough time is allowed to see if the patient recovers normal conduction.
Pathophysiological Mechanism of Vagal response during Inferior MI:
There is limited consensus as to the exact mechanisms which mediate this vagal phenomena during inferior MI’s however, some proposed mechanisms include:
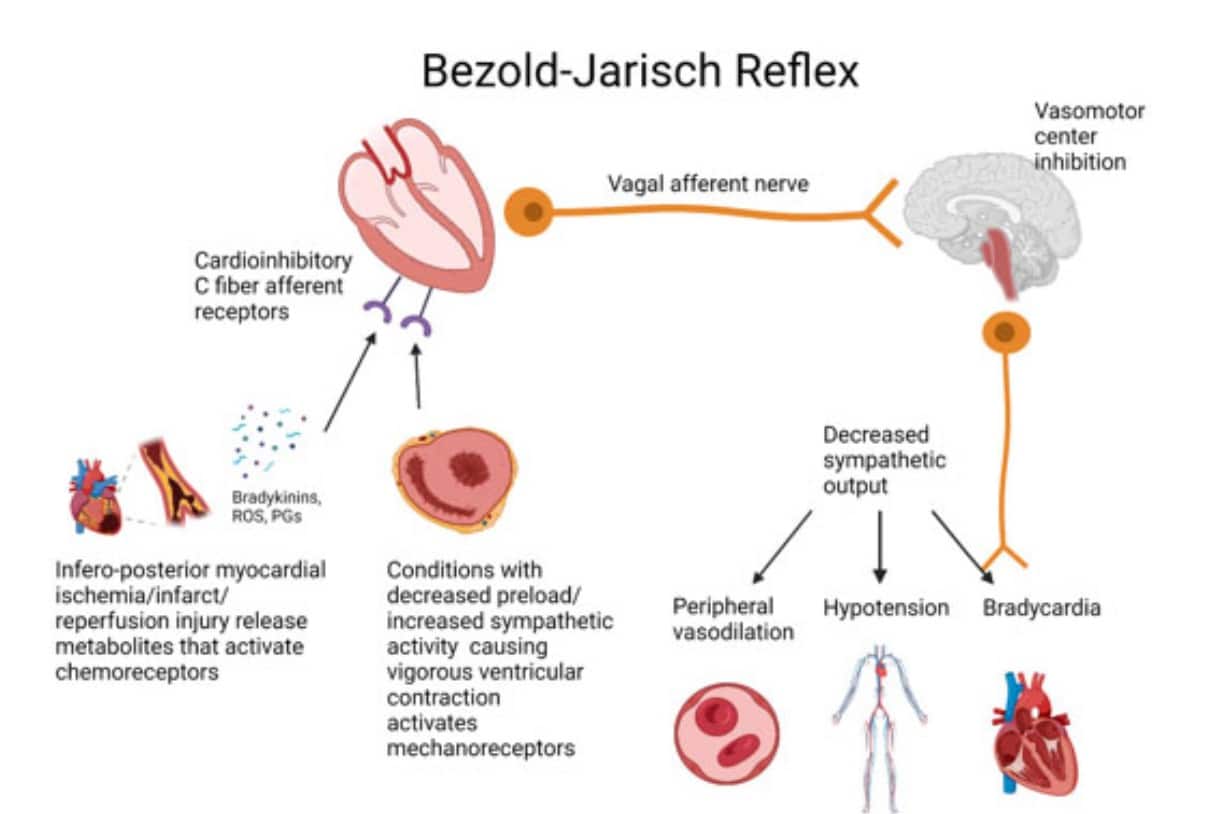
1. Bezold-Jarisch Reflex
The inferior wall of the LV, supplied by the RCA has a higher density of vagal nerve fibres. Ischemia stimulates these fibres (called the Bezold-Jarisch Reflex) making the reflex more pronounced during inferior ischemia compared to other territory infarcts.
Inferior ischemia can stimulate mechanoreceptors and chemoreceptors which send afferent signals via vagal fibers to the brainstem.
Once received by the brainstem, it triggers a vagal response via the vagus nerve. This results in SA nodal bradycardia, slowed conduction velocity in the AV node (prolonged PR interval) and AV block. Peripherally, it can contribute to vasodilation & hypotension, causing the patient to feel light headed, diaphoretic, weak & nauseous.
2. Ganglionic Plexi ischemia
Ganglionic Plexi associated with vagal mediated phenomena are located in the posterior basal portion of the inter-atrial septum. Dominant RCA’s &/or Left Circumflex usually supply this. When these vessels are obstructed, these structures are also rendered ischemic along with the inferior wall. Ischemic injury to these structures affects their autonomic regulation of the heart & may result in sinus bradycardia and peripheral vasodilation.
3. RV Ischemia
RV involvement during proximal RCA obstruction can result in a hypokinetic RV, which fails to propel blood forward, reducing CO & triggering systemic hypotension & result in vagal-like symptoms.
My two cents:
Inferior MI is often associated with vagal phenomena, including systemic hypotension & bradyarrhythmias, including sinus arrest & 3rd degree AV block.
This vagal phenomena is likely mediated by an increased density of vagal afferent fibres on the inferior wall of the LV, as well as acute RV ischemia mediating a pronounced Central Nervous System vagal response, resulting in peripheral hypotension & bradyarrhythmias.
Bradyarrhythmias associated with Inferior MI’s are rarely permanent & usually recover within 2 weeks.
Concerted effort should be made to resist the temptation to immediately implant a Permanent Pacemaker in this setting (“OculoPacing Reflex!”). – “Give Peace a Chance”.
Thanks for tuning in :)
Cheers
Mitch & CPP Team
Myocardial Infarction & it’s associated ECG features & bradyarrhythmias is discussed in more detail in ECG in Practice
References:
Tan JW, Parekh J, Shukla A. Bradyarrhythmia in acute massive pulmonary embolism. Int J Case Rep Images 2023;14(1):47–51.
Zandstra TE, Notenboom RGE, Wink J, Kiès P, Vliegen HW, Egorova AD, Schalij MJ, De Ruiter MC, Jongbloed MRM. Asymmetry and Heterogeneity: Part and Parcel in Cardiac Autonomic Innervation and Function. Front Physiol. 2021 Sep 16;12:665298.
Trappe H. J. (2010). Tachyarrhythmias, bradyarrhythmias and acute coronary syndromes. Journal of emergencies, trauma, and shock, 3(2), 137–142. https://doi.org/10.4103/0974-2700.62112
Singh SM, FitzGerald G, Yan AT, et al. High-grade atrioventricular block in acute coronary syndromes: insights from the Global Registry of Acute Coronary Events. Eur Heart J. 2015;36(16):976-983.
Thadathilankal-Jess John, Charles Kyriakakis, Don Zachariah, Anton Doubell, Inferior ST-elevation myocardial infarction managed with a pharmacoinvasive strategy and conservative management of delayed atrioventricular block: classical case report, European Heart Journal – Case Reports, Volume 4, Issue 6, December 2020, Pages 1–7,
Aplin M, Engstrøm T, Vejlstrup NG, et al. Prognostic importance of complete atrioventricular block complicating acute myocardial infarction. Am J Cardiol. 2003;92(7):853-856.
Rotman M, Wagner GS, Wallace AG. Bradyarrhythmias in acute myocardial infarction. Circulation. 1972;45(3):703-722.
James TN: Cardiac innervation: Anatomic and pharmacologic relationships. Bull N Y Acad Med 43: 1041, 1967
Flapan AD, Wright RA, Nolan J, Neilson JM, Ewing DJ. Differing patterns of cardiac parasympathetic activity and their evolution in selected patients with a first myocardial infarction. J Am Coll Cardiol. 1993 Mar 15;21(4):926-31.
Perez-Gomez F, Martin de Dios R, Rey J, Garcia Aguado A. Prinzmetal’s angina:reflex cardiovascular response during episode