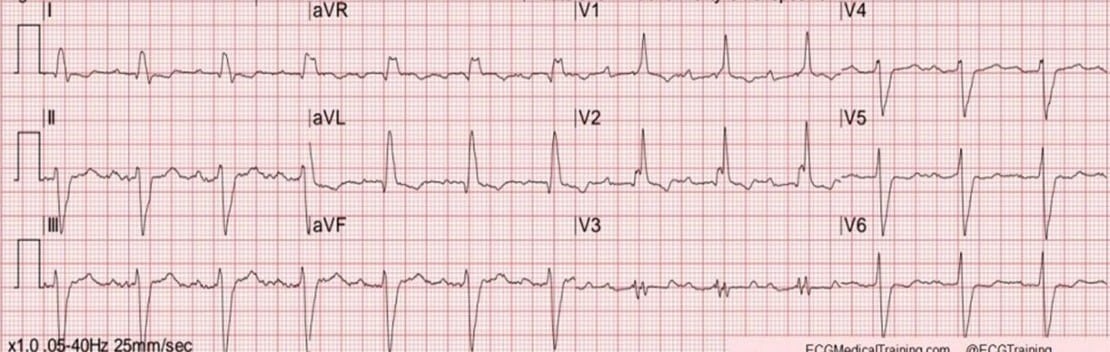
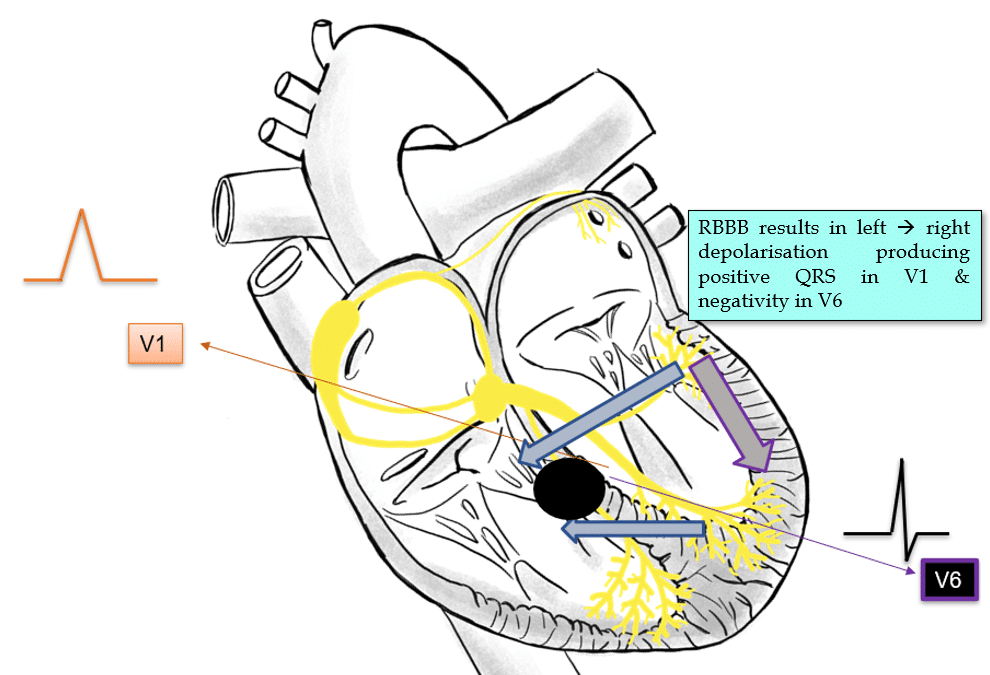
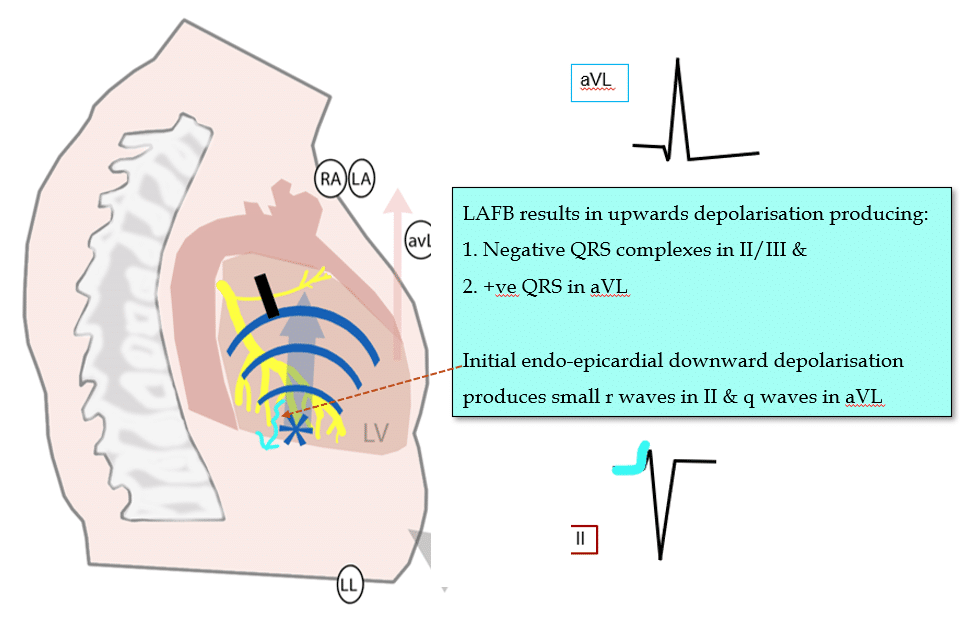
Answer: Sinus rhythm with RBBB, Left axis, 1st degree AV conduction delay & Left Anterior Fascicular Block. (So-called “Trifascicular block” – please don’t use that term. It’s misleading).
Evidence of disease in multiple locations, impacting the function of the cardiac conduction system. Given her history of falls & dizzy spells, there are strong reasons to be concerned about the possibility of intermittent conduction system failure (resulting in complete heart block, or ventricular standstill or high grade 2nd degree AV block) causing her symptoms.
Her ECG features of note are:
My two cents:
Bi-fascicular block with 1st-degree AV conduction delay (often called “trifascicular block”) in the context of unexplained syncope strongly suggests a cardiac cause due to the high likelihood of severe His-Purkinje disease.
These findings warrant further investigation with an EP study to assess the His-Purkinje disease burden or consider pacemaker implantation.
Cheers
Mitch & CPP Team
P.s. This ECG was actually from a 77 year old male. I realised after I posted the blog. It doesn’t change the lessons learnt, but I wanted to set the record straight for the sake of correctness :)