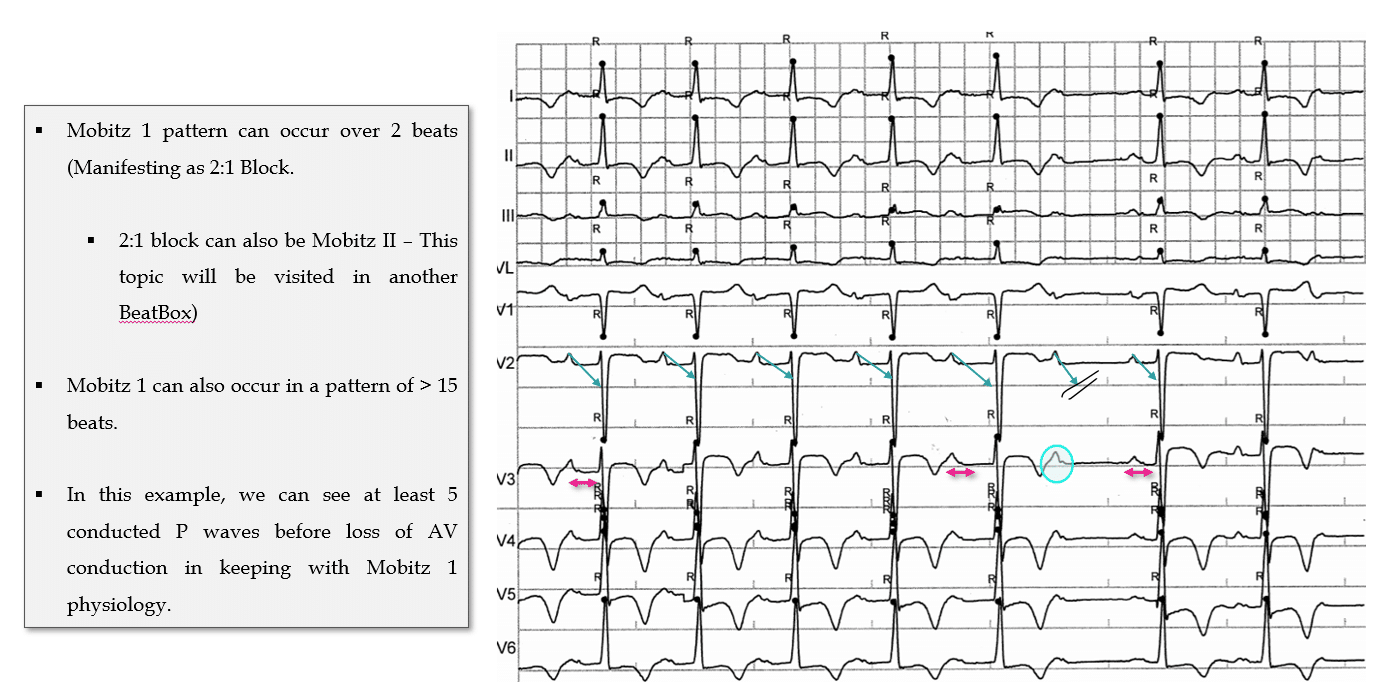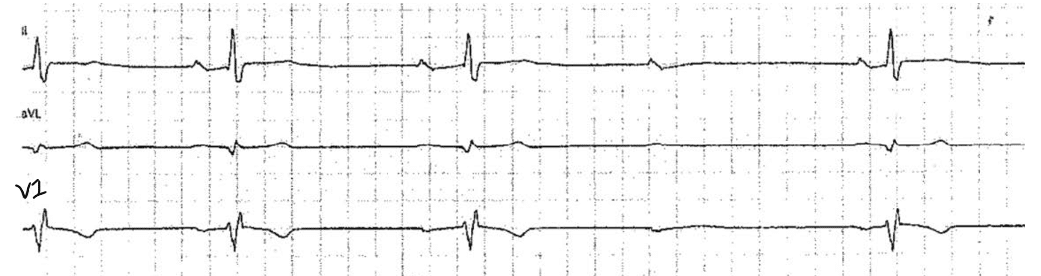
Answer: Sinus Rhythm with 2nd degree AV Block, Mobitz 1, driven by high parasympathetic (vagal) tone.
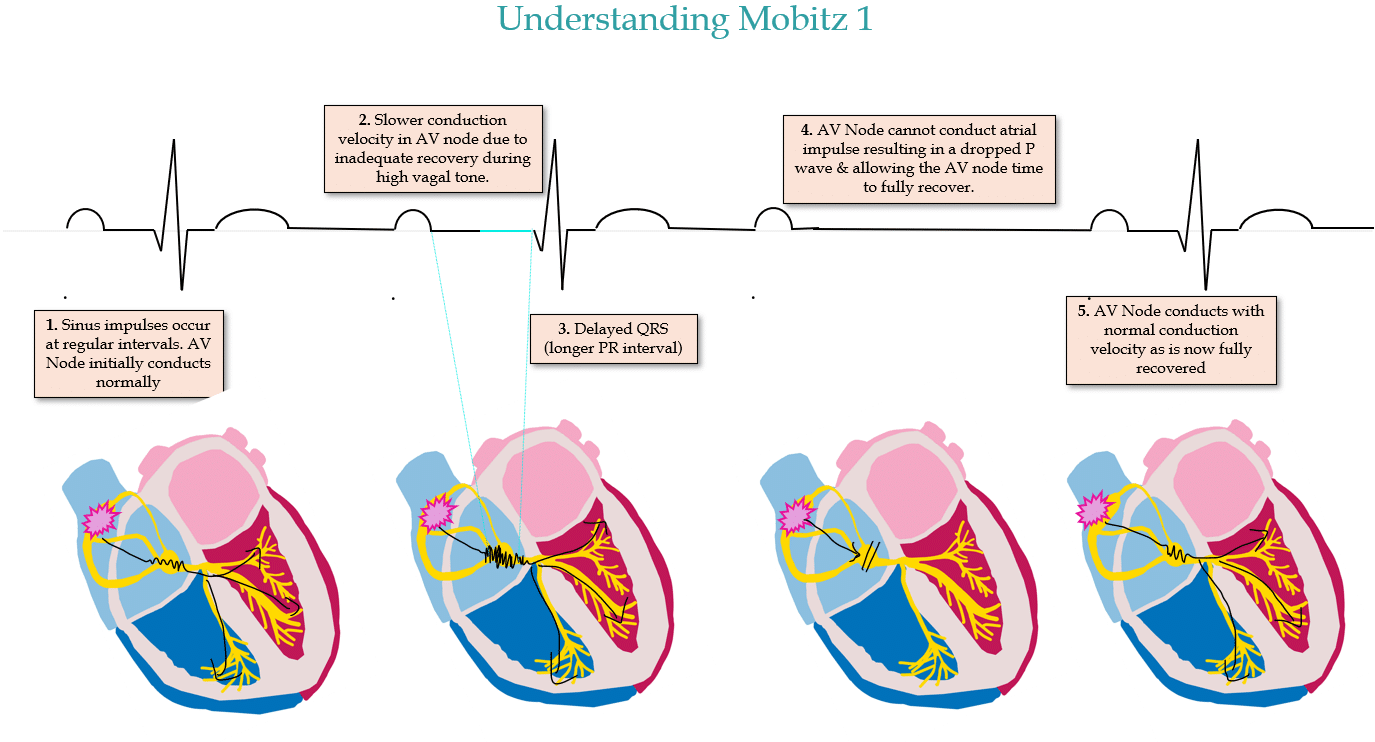
Progressively lengthening PR interval followed by a non conducted P wave.
The subsequent conducted P wave will then have a PR interval that is shorter than the last conducted PR interval prior to the non conducted beat.
CONTEXT is everything:
My Two Cents:
Thanks for tuning in :)
Cheers
Mitch & CPP Team
Learn more about Bradyarrhythmias in our ECG in Practice – Program 1